Fri, Apr 26, 2024
Volume 7, Issue 3 (9-2018)
2018, 7(3): 129-136 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Talatof Z, Behbahanirad A, Arazi A, Azad A. Reliability and Reproducibility of the International Caries Detection and Assessment System Index in Evaluation of Dental Decay in People Aged 25-40 Years. Journal title 2018; 7 (3) :129-136
URL: http://3dj.gums.ac.ir/article-1-325-en.html
URL: http://3dj.gums.ac.ir/article-1-325-en.html



1- Assistant professor, Department of Oral and Maxillofacial Medicine, Shool of Dentistry, Shiraz Branch, Islamic Azad University, Shiraz, Iran.
2- Assistant Professor, Department of Dental Public Health, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
3- Dentistry Student Research Committee, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
4- Assistant Professor, Dental Disease Research Center, Department of Oral and Maxillofacial Medicine, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
2- Assistant Professor, Department of Dental Public Health, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
3- Dentistry Student Research Committee, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
4- Assistant Professor, Dental Disease Research Center, Department of Oral and Maxillofacial Medicine, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
Keywords: Dental Caries, Reproducibility of results, Students, Dental Cross- Sectional Studies, Education, Dental
Full-Text [PDF 775 kb]
(745 Downloads)
| Abstract (HTML) (2376 Views)



Full-Text: (839 Views)
1. Introduction
ental decay is one of the most prevalent chronic diseases, which involves all human societies with different intensities. This disease imposes a financial burden to people and society at the personal and governmental levels. Dental indices can be considered as the main tools for the investigations related to epidemiology in patients to find out the prevalence and intensity of oral diseases. Moreover, prevention programs are based on dental indices for oral health promotion. Dental indices allow dentists to evaluate the advantages of more recent dental treatment methods in comparison with the available old methods [1].
Indices such as Decay-Missing-Filled Teeth (DMFT) and Decay-Missing-Filled Surface (DMFS) have been used for a long time in epidemiologic studies for evaluating dental decay by calculating the number of D: represents Decayed (D), Missing (M), and Filled (F), Teeth (T) or Surface (S). Lowercase letters (dmft and dmfs) are used to denote evaluating the deciduous teeth, and uppercase letters (DMFT and DMFS) for assessing the permanent teeth. These indices are the most common epidemiologic surveys of dental decay [2]. Based on the evidences presented on the DMT index so far, this criterion has acceptable reliability and reproducibility to be used by dentists and dental students [3].
One main factor contributing to the high prevalence of caries is the lack of recording the stages of dental decay and not finding the decay in the early stages for on-time prevention. Moreover, lack of coordination in the informational system at national and international levels may have destructive impacts on caries prevention programs. These difficulties led to cumulative efforts to design and propose a unified method, called the International Caries Detection and Assessment System (ICDAS) and establishing a unit committee (ICDAS committee) in 2002 to be used all over the world for recording dental decays [4]. In this method, the codes ranging from 0 to 6 are considered for the decay condition of each tooth from the beginning of enamel decalcification to advanced decays. In the ICDAS system, crown decays and those associated with restorations and sealants have different codes. This method has some advantages including identifying intensity, activity or inactivity of dental decays and the possibility of comparing the results of various studies conducted in different countries with higher accuracy [5, 6].
Several studies applied the ICDAS index in their communities to assess its validity and reliability [7]. In 2015, Goswami and Rajwar concluded that the ICDAS index had good potential as the traditional method of World Health Organization (WHO) for examining dental decays [8]. Aidara and Bourgeois declared that the ICDAS index provided 43% information more than the DMF. Therefore, ICDAS index demonstrated more prevention needs in comparison to DMF [9]. The results of other studies such as Ismail et al. and Shoaib et al. showed that these diagnosis criteria had the required validity for application [10, 11].
To our best knowledge, most of previous studies have reported the use of ICDAS on extracted teeth [12-15], but few studies have assessed the ICDAS on patients [11, 16]. Moreover, the ICDAS index is not taught and used in dental schools of Iran and dental examination is still carried out using the DMF index. Therefore, assessing the ICDAS index in Iran seems essential to integrate it into our national oral health promotion programs. In this regard, the aim of this study was to investigate the reliability and reproducibility of the ICDAS index.
2. Materials and Methods
In this cross-sectional study, 30 employees aged 25-40 years working in the Nader Kazemi Hospital, Shiraz, Iran were selected as study subjects, using the convenience sampling method. Those who were edentulous, had limitations in opening their mouth or had orthodontics brackets, were excluded from the study and replaced by other subjects. Research objective and method were completely explained to the subjects. The all participated in the study voluntarily and with full informed consent. Permission was obtained from the Dental School of Shiraz University of Medical Sciences.
Two dental students that were chosen as examiners were calibrated by a dentist in Kerman University who was the only person calibrated for this index by the ICDAS committee in Iran. First, description of this index including the introduction, the way of using and its codes were instructed to them. Then, diagnosis pictures were presented to them and finally, the they were tested based on the ICDAS rules. After passing the exam, their ICDAS knowledge was examined on extracted teeth and approved by the specialist. The two other dental students were calibrated for DMF index in their educational setting.
Two examiners recorded the DMF index and the two other examiners recorded the ICDAS index on different days to have no idea about the results of each other. Two weeks later, all examinations were repeated by one of the former examiners for DMF and ICDAS indices. Examinations were performed on dental units using a dental mirror and a WHO periodontal probe. Before the examination, subjects cleaned their teeth using a toothbrush. The number of Decayed teeth (D), Missed teeth (M), and Filled teeth (F) were recorded in the DMF form.
In the ICDAS form, based on the instruction published by ICDAS Committee, the condition of teeth at occlusal and plane levels were examined and recorded at both moist and dry states (air-dried for 5 s), according to the codes presented in tables 1 and 2. In the ICDAS system the condition of each tooth is specified by a tow-digit code, the left digit was recorded by determining the condition of each tooth as follows: 0= Sound; 1= First visual change in enamel seen after drying; 2= Distinct visual change in enamel; 3= Localized enamel breakdown; 4= Underlying dark shadow from dentine; 5= Distinct cavity with visible dentine; and 6= Extensive distinct cavity with visible dentine. The right digit was recorded according to Table 2 where the tooth condition is scored from 0 to 9; 0 indicates an intact tooth and other codes [1-9] show teeth with various restorations or tooth losing.
ental decay is one of the most prevalent chronic diseases, which involves all human societies with different intensities. This disease imposes a financial burden to people and society at the personal and governmental levels. Dental indices can be considered as the main tools for the investigations related to epidemiology in patients to find out the prevalence and intensity of oral diseases. Moreover, prevention programs are based on dental indices for oral health promotion. Dental indices allow dentists to evaluate the advantages of more recent dental treatment methods in comparison with the available old methods [1].
Indices such as Decay-Missing-Filled Teeth (DMFT) and Decay-Missing-Filled Surface (DMFS) have been used for a long time in epidemiologic studies for evaluating dental decay by calculating the number of D: represents Decayed (D), Missing (M), and Filled (F), Teeth (T) or Surface (S). Lowercase letters (dmft and dmfs) are used to denote evaluating the deciduous teeth, and uppercase letters (DMFT and DMFS) for assessing the permanent teeth. These indices are the most common epidemiologic surveys of dental decay [2]. Based on the evidences presented on the DMT index so far, this criterion has acceptable reliability and reproducibility to be used by dentists and dental students [3].
One main factor contributing to the high prevalence of caries is the lack of recording the stages of dental decay and not finding the decay in the early stages for on-time prevention. Moreover, lack of coordination in the informational system at national and international levels may have destructive impacts on caries prevention programs. These difficulties led to cumulative efforts to design and propose a unified method, called the International Caries Detection and Assessment System (ICDAS) and establishing a unit committee (ICDAS committee) in 2002 to be used all over the world for recording dental decays [4]. In this method, the codes ranging from 0 to 6 are considered for the decay condition of each tooth from the beginning of enamel decalcification to advanced decays. In the ICDAS system, crown decays and those associated with restorations and sealants have different codes. This method has some advantages including identifying intensity, activity or inactivity of dental decays and the possibility of comparing the results of various studies conducted in different countries with higher accuracy [5, 6].
Several studies applied the ICDAS index in their communities to assess its validity and reliability [7]. In 2015, Goswami and Rajwar concluded that the ICDAS index had good potential as the traditional method of World Health Organization (WHO) for examining dental decays [8]. Aidara and Bourgeois declared that the ICDAS index provided 43% information more than the DMF. Therefore, ICDAS index demonstrated more prevention needs in comparison to DMF [9]. The results of other studies such as Ismail et al. and Shoaib et al. showed that these diagnosis criteria had the required validity for application [10, 11].
To our best knowledge, most of previous studies have reported the use of ICDAS on extracted teeth [12-15], but few studies have assessed the ICDAS on patients [11, 16]. Moreover, the ICDAS index is not taught and used in dental schools of Iran and dental examination is still carried out using the DMF index. Therefore, assessing the ICDAS index in Iran seems essential to integrate it into our national oral health promotion programs. In this regard, the aim of this study was to investigate the reliability and reproducibility of the ICDAS index.
2. Materials and Methods
In this cross-sectional study, 30 employees aged 25-40 years working in the Nader Kazemi Hospital, Shiraz, Iran were selected as study subjects, using the convenience sampling method. Those who were edentulous, had limitations in opening their mouth or had orthodontics brackets, were excluded from the study and replaced by other subjects. Research objective and method were completely explained to the subjects. The all participated in the study voluntarily and with full informed consent. Permission was obtained from the Dental School of Shiraz University of Medical Sciences.
Two dental students that were chosen as examiners were calibrated by a dentist in Kerman University who was the only person calibrated for this index by the ICDAS committee in Iran. First, description of this index including the introduction, the way of using and its codes were instructed to them. Then, diagnosis pictures were presented to them and finally, the they were tested based on the ICDAS rules. After passing the exam, their ICDAS knowledge was examined on extracted teeth and approved by the specialist. The two other dental students were calibrated for DMF index in their educational setting.
Two examiners recorded the DMF index and the two other examiners recorded the ICDAS index on different days to have no idea about the results of each other. Two weeks later, all examinations were repeated by one of the former examiners for DMF and ICDAS indices. Examinations were performed on dental units using a dental mirror and a WHO periodontal probe. Before the examination, subjects cleaned their teeth using a toothbrush. The number of Decayed teeth (D), Missed teeth (M), and Filled teeth (F) were recorded in the DMF form.
In the ICDAS form, based on the instruction published by ICDAS Committee, the condition of teeth at occlusal and plane levels were examined and recorded at both moist and dry states (air-dried for 5 s), according to the codes presented in tables 1 and 2. In the ICDAS system the condition of each tooth is specified by a tow-digit code, the left digit was recorded by determining the condition of each tooth as follows: 0= Sound; 1= First visual change in enamel seen after drying; 2= Distinct visual change in enamel; 3= Localized enamel breakdown; 4= Underlying dark shadow from dentine; 5= Distinct cavity with visible dentine; and 6= Extensive distinct cavity with visible dentine. The right digit was recorded according to Table 2 where the tooth condition is scored from 0 to 9; 0 indicates an intact tooth and other codes [1-9] show teeth with various restorations or tooth losing.
Statistical analysis was performed in SPSS v. 18 software. The Kappa coefficient was used to investigate inter‐ and intra‐examiner reproducibility. According to Cohen, Kappa values ≤0 shows no agreement; 0.01-0.20, none to slight; 0.21-0.40, fair; 0.41-0.60, moderate; 0.61-0.80 substantial; and 0.81-1.00, almost perfect agreement [17].
3. Results
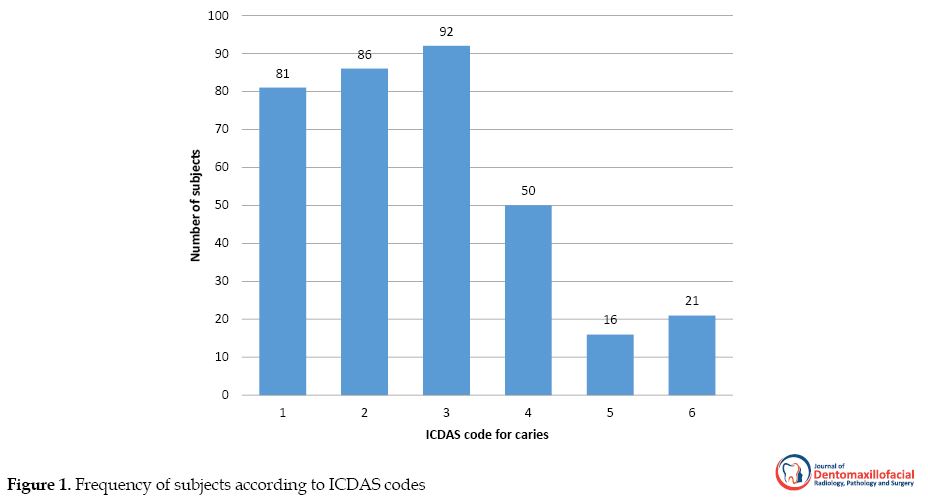
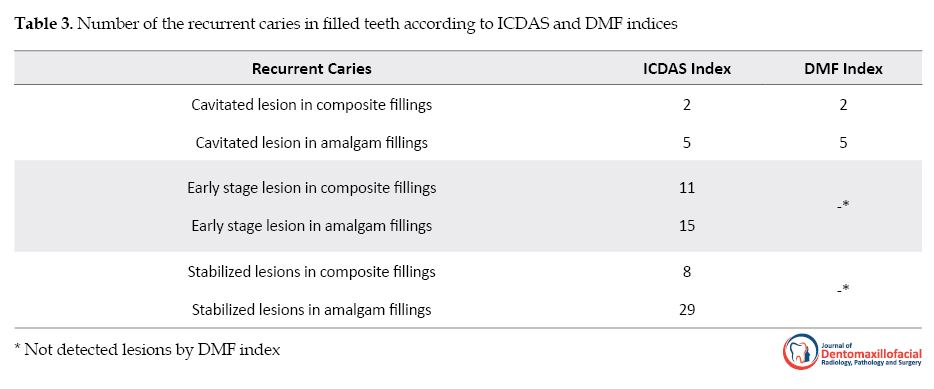
Thirty subjects (20 women and 10 men) participated in this study with the mean age of 28 years. The total number of lost teeth was 119 of which 59 lost due to reasons other than caries, 47 because of caries, and 13 teeth had no eruption. According to DMF index, the total number of filled teeth among subjects was 129 of which 26 had composite filling and 104 had amalgam filling. The total number of decayed teeth based on this index was 37. According to ICDAS index, 346 teeth were considered as decayed teeth. The frequency of subjects based on ICDAS codes is shown in Figure 1, and the distribution of recurrent caries in filled teeth based on ICDAS and DMF indices is shown in Table 3.
3. Results
Thirty subjects (20 women and 10 men) participated in this study with the mean age of 28 years. The total number of lost teeth was 119 of which 59 lost due to reasons other than caries, 47 because of caries, and 13 teeth had no eruption. According to DMF index, the total number of filled teeth among subjects was 129 of which 26 had composite filling and 104 had amalgam filling. The total number of decayed teeth based on this index was 37. According to ICDAS index, 346 teeth were considered as decayed teeth. The frequency of subjects based on ICDAS codes is shown in Figure 1, and the distribution of recurrent caries in filled teeth based on ICDAS and DMF indices is shown in Table 3.
Based on ICDAS index, 70 recurrent caries were detected of which 63 were non-cavitated, while only 7 cavitated caries lesions were detected by DMF index. The intra-examiner and the inter-examiner Kappa coefficients for the ICDAS and DMF indices are shown in Table 4 (P<0.001). Therefore, according to Cohen [17], there is an almost perfect agreement between intra- and inter-examiners.
4. Discussion
In present study, teeth were examined by both DMF and ICDAS indices. Based on the DMF index, 37 teeth were considered as carious teeth. However, the ICDAS index showed 346 teeth as carious teeth. Considering cavitated lesions, the ICDAS index (codes 5 and 6) revealed similar results to those of the DMF index. As expected, the ICDAS index could demonstrate the stages, depth, and type of carious lesions in examined teeth. The number of recurrent caries using DMF and ICDAS criteria was 7 and 70, respectively.
The Kappa coefficients for inter- and intra-examiner agreement for DMF index were 0.83 and 0.90 and the values for ICDAS index were 0.87 and 0.91, respectively. According to Cohen [17], these values are in almost perfect ranges. Therefore, following proper training of dental students, the ICDAS index seems to be a reliable and reproducible index. Several studies have been performed worldwide to assess the reliability and reproducibility of this index. Some of these studies merely performed in vitro [12-14]. To use the ICDAS index in epidemiological studies, its assessment in human subjects is the next step. Jablonski-Momeni et al. in 2008 assessed the ICDAS index in 100 extracted teeth among four dentists. They found the Kappa values for inter- and intra-examiner reproducibility were 0.62-0.83. Although their results were in the acceptable range, our findings reported higher kappa values. Examining the extracted teeth may be the reason for the different outcomes in comparison to human subjects’ examinations.
In another study in 2015 in New Delhi, 31 children aged between 3-14 years were examined using the WHO method and the ICDAS index. It was concluded that the ICDAS index had a potential similar to the WHO method in examining dental decays [8]. Braga et al. [18] reported a Kappa coefficient of 0.91 for the ICDAS index on the primary molars extracted in children. Although they performed the study in children, their results were in line with the current study.
A recent study in 2019 was performed by five dentists using ICDAS index, on 270 extracted permanent premolars and molars [15]. The kappa coefficient for inter-examiner reproducibility ranged 0.50-0.68 indicating a moderate agreement. Higher values reported in our study may be due to fewer numbers of examiners (two).
We assessed the human samples in this study, while in vitro samples were examined in the most of previous studies. So the results could be more applicable than in vitro studies. Most of the teeth with carious lesions detected by the ICDAS criteria in the current study, were classified as code 3. This implies the importance of early caries detection for developing minimal intervention dentistry. These lesions were not detected by the DMF index. Hence, applying the ICDAS criteria seems to be an advantage for this system over traditional systems. Moreover, preventive programs can be performed for these teeth in the early stages.
The number of non-cavitated recurrent caries lesions detected in the present study by ICDAS were 63, while by DMF index, only sevencavitated recurrent caries lesion were identified. Therefore, early detection of non-cavitated recurrent lesions is another advantage for the ICDAS index which can prevent further aggressive treatments. The examiners were evaluated using extracted teeth prior to the study. So, the calibration was performed well in this study. Moreover, the examiners were unaware of the records of each other.
Further studies should be performed with a larger sample size. In Iran, the ICDAS index is not commonly taught in dental schools; therefore, we had difficulties in educating and calibration of examiners. In this regard, the examiners inevitably traveled to Kerman city to calibrate for this index.
Less studies have been performed in Iran on applying the ICDAS index; hence, further studies should be designed with a larger sample size and more calibrated examiners across the country. Dentists should be trained for applying the ICDAS index in diagnosing dental caries. If this system performed well, preventive dental care can lead to minimal intervention dentistry. Most of the carious teeth classified as code 1 to 4 in ICDAS can be arrested and rematerialized as sound teeth by applying on-time preventive programs. Therefore, integration of this system criteria in the dental curriculum can be beneficial to promote oral health. Moreover, ICDAS system can be applied in future epidemiological studies.
5. Conclusion
The ICDAS index was feasible for dental students following proper training. The reliability and reproducibility of ICDAS and DMF indices were great. Hence, it can provide appropriate information to arrest the early carious lesions by preventive programs.
Ethical Considerations
Compliance with ethical guidelines
The all participated in the study voluntarily and with full informed consent. Permission was obtained from the Dental School of Shiraz University of Medical Sciences (Number Grant. 8894136).
Funding
this article was based on the PhD. thesis from Aida Arazi in Department of Oral and Maxillofacial Medicine , School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran. This research was conducted by the support of Vice-Chancellory of Research Shiraz University of Medical Science for supporting this research (Number Grant: 8894136).
Authors contribution's
Conceptualization: all authors; Methodology: Zahra Talattof, Aida Arazi; Investigation: all authors; Writing -original draft: all authors; Writing-review & editing: Arghavan Behbahanirad, Azita Azad; Supervision: Azita Azad, Arghavan Behbahanirad.
Conflict of interest
There are no conflicts of interest to declare.
Acknowledgements
The authors thank the Vice-Chancellory of Research Shiraz University of Medical Science for supporting this research. The authors also thank Dr. Mehrdad Vossoughi of the Dental Research Development center, of the school of Dentistry for the statistical analysis.
References
In present study, teeth were examined by both DMF and ICDAS indices. Based on the DMF index, 37 teeth were considered as carious teeth. However, the ICDAS index showed 346 teeth as carious teeth. Considering cavitated lesions, the ICDAS index (codes 5 and 6) revealed similar results to those of the DMF index. As expected, the ICDAS index could demonstrate the stages, depth, and type of carious lesions in examined teeth. The number of recurrent caries using DMF and ICDAS criteria was 7 and 70, respectively.
The Kappa coefficients for inter- and intra-examiner agreement for DMF index were 0.83 and 0.90 and the values for ICDAS index were 0.87 and 0.91, respectively. According to Cohen [17], these values are in almost perfect ranges. Therefore, following proper training of dental students, the ICDAS index seems to be a reliable and reproducible index. Several studies have been performed worldwide to assess the reliability and reproducibility of this index. Some of these studies merely performed in vitro [12-14]. To use the ICDAS index in epidemiological studies, its assessment in human subjects is the next step. Jablonski-Momeni et al. in 2008 assessed the ICDAS index in 100 extracted teeth among four dentists. They found the Kappa values for inter- and intra-examiner reproducibility were 0.62-0.83. Although their results were in the acceptable range, our findings reported higher kappa values. Examining the extracted teeth may be the reason for the different outcomes in comparison to human subjects’ examinations.
In another study in 2015 in New Delhi, 31 children aged between 3-14 years were examined using the WHO method and the ICDAS index. It was concluded that the ICDAS index had a potential similar to the WHO method in examining dental decays [8]. Braga et al. [18] reported a Kappa coefficient of 0.91 for the ICDAS index on the primary molars extracted in children. Although they performed the study in children, their results were in line with the current study.
A recent study in 2019 was performed by five dentists using ICDAS index, on 270 extracted permanent premolars and molars [15]. The kappa coefficient for inter-examiner reproducibility ranged 0.50-0.68 indicating a moderate agreement. Higher values reported in our study may be due to fewer numbers of examiners (two).
We assessed the human samples in this study, while in vitro samples were examined in the most of previous studies. So the results could be more applicable than in vitro studies. Most of the teeth with carious lesions detected by the ICDAS criteria in the current study, were classified as code 3. This implies the importance of early caries detection for developing minimal intervention dentistry. These lesions were not detected by the DMF index. Hence, applying the ICDAS criteria seems to be an advantage for this system over traditional systems. Moreover, preventive programs can be performed for these teeth in the early stages.
The number of non-cavitated recurrent caries lesions detected in the present study by ICDAS were 63, while by DMF index, only sevencavitated recurrent caries lesion were identified. Therefore, early detection of non-cavitated recurrent lesions is another advantage for the ICDAS index which can prevent further aggressive treatments. The examiners were evaluated using extracted teeth prior to the study. So, the calibration was performed well in this study. Moreover, the examiners were unaware of the records of each other.
Further studies should be performed with a larger sample size. In Iran, the ICDAS index is not commonly taught in dental schools; therefore, we had difficulties in educating and calibration of examiners. In this regard, the examiners inevitably traveled to Kerman city to calibrate for this index.
Less studies have been performed in Iran on applying the ICDAS index; hence, further studies should be designed with a larger sample size and more calibrated examiners across the country. Dentists should be trained for applying the ICDAS index in diagnosing dental caries. If this system performed well, preventive dental care can lead to minimal intervention dentistry. Most of the carious teeth classified as code 1 to 4 in ICDAS can be arrested and rematerialized as sound teeth by applying on-time preventive programs. Therefore, integration of this system criteria in the dental curriculum can be beneficial to promote oral health. Moreover, ICDAS system can be applied in future epidemiological studies.
5. Conclusion
The ICDAS index was feasible for dental students following proper training. The reliability and reproducibility of ICDAS and DMF indices were great. Hence, it can provide appropriate information to arrest the early carious lesions by preventive programs.
Ethical Considerations
Compliance with ethical guidelines
The all participated in the study voluntarily and with full informed consent. Permission was obtained from the Dental School of Shiraz University of Medical Sciences (Number Grant. 8894136).
Funding
this article was based on the PhD. thesis from Aida Arazi in Department of Oral and Maxillofacial Medicine , School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran. This research was conducted by the support of Vice-Chancellory of Research Shiraz University of Medical Science for supporting this research (Number Grant: 8894136).
Authors contribution's
Conceptualization: all authors; Methodology: Zahra Talattof, Aida Arazi; Investigation: all authors; Writing -original draft: all authors; Writing-review & editing: Arghavan Behbahanirad, Azita Azad; Supervision: Azita Azad, Arghavan Behbahanirad.
Conflict of interest
There are no conflicts of interest to declare.
Acknowledgements
The authors thank the Vice-Chancellory of Research Shiraz University of Medical Science for supporting this research. The authors also thank Dr. Mehrdad Vossoughi of the Dental Research Development center, of the school of Dentistry for the statistical analysis.
References
- Pitts N. Modern concepts of caries measurement. Journal of dental research. 2004; 83(1_suppl):43-7. [DOI:10.1177/154405910408301s09] [PMID]
- Heymann HO, Swift JrEJ, Ritter AV. Sturdevant’s art & science of operative dentistry-e-book: Amsterdam: Elsevier Health Sciences; 2014.
- Pereira SM, Tagliaferro EPdS, Cortellazzi KL, Ambrosano GMB, Mialhe FL, Meneghim MdC, et al. Estimate of DMF index using teeth most affected by dental caries in twelve-year-old children. Revista de Saude Publica. 2009; 43(1):179-82. [DOI:10.1590/S0034-89102009000100024] [PMID]
- Nyvad B, Machiulskiene V, Bælum V. Construct and predictive validity of clinical caries diagnostic criteria assessing lesion activity. Journal of Dental Research. 2003; 82(2):117-22. [DOI:10.1177/154405910308200208] [PMID]
- Dikmen B. Icdas II criteria (international caries detection and assessment system). Journal of Istanbul University Shool of Dentistry. 2015; 49(3):63-72. [DOI:10.17096/jiufd.38691] [PMID] [PMCID]
- Banting D, Eggertsson H, Ekstrand K, Ferreira-Zandoná A, Ismail A, Longbottom C, et al. Rationale and evidence for the International Caries Detection and Assessment System (ICDAS II). Ann Arbor. 2005; 1001:48109-1078.
- Jablonski-Momeni A, Ricketts DN, Heinzel-Gutenbrunner M, Stoll R, Stachniss V, Pieper K. Impact of scoring single or multiple occlusal lesions on estimates of diagnostic accuracy of the visual ICDAS-II system. International journal of Dentistry. 2009; 2009. [DOI:10.1155/2009/798283] [PMID] [PMCID]
- Goswami M, Rajwar AS. Evaluation of cavitated and non-cavitated carious lesions using the WHO basic methods, ICDAS-II and laser fluorescence measurements. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2015; 33(1):10. [DOI:10.4103/0970-4388.148961] [PMID]
- Aidara A, Bourgeois D. Prevalence of dental caries: national pilot study comparing the severity of decay (CAO) vs ICDAS index in Senegal. Odonto-stomatologie tropicale= Tropical dental journal. 2014; 37(145):53-63.
- Shoaib L, Deery C, Ricketts D, Nugent Z. Validity and reproducibility of ICDAS II in primary teeth. Caries research. 2009; 43(6):442-8. [DOI:10.1159/000258551] [PMID]
- Ismail A, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community dentistry and oral epidemiology. 2007; 35(3):170-8. [DOI:10.1111/j.1600-0528.2007.00347.x] [PMID]
- Jablonski-Momeni A, Stachniss V, Ricketts DN, Heinzel-Gutenbrunner M, Pieper K. Reproducibility and accuracy of the ICDAS-II for detection of occlusal caries in vitro. Caries research. 2008; 42(2):79-87. [DOI:10.1159/000113160] [PMID]
- Zandona AGF, Al-Shiha S, Eggertsson H, Eckert G. Student versus Shool performance using a new visual criteria for the detection of caries on occlusal surfaces: an in vitro examination with histological validation. Operative Dentistry. 2009; 34(5):598-604. [DOI:10.2341/08-082-L] [PMID]
- Ekstrand KR, Luna LE, Promisiero L, Cortes A, Cuevas S, Reyes JF, et al. The reliability and accuracy of two methods for proximal caries detection and depth on directly visible proximal surfaces: An in vitro study. Caries Research. 2011; 45(2):93-9. [DOI:10.1159/000324439] [PMID]
- Qudeimat MA, Altarakemah Y, Alomari Q, Alshawaf N, Honkala E. The impact of ICDAS on occlusal caries treatment recommendations for high caries risk patients: An in vitro study. BMC Oral Health. 2019; 19(1):41. [DOI:10.1186/s12903-019-0730-8] [PMID] [PMCID]
- Cadavid AS, Lince CMA, Jaramillo MC. Dental caries in the primary dentition of a Colombian population according to the ICDAS criteria. Brazilian Oral Research. 2010; 24(2):211-6. [DOI:10.1590/S1806-83242010000200014] [PMID]
- Cohen J. A coefficient of agreement for nominal scales. Educational and Psychological Measurement. 1960; 20(1):37-46. [DOI:10.1177/001316446002000104]
- Braga MM, Ekstrand KR, Martignon S, Imparato JCP, Ricketts DNJ, Mendes FM. Clinical performance of two visual scoring systems in detecting and assessing activity status of occlusal caries in primary teeth. Caries Research. 2010; 44(3):300-8. [DOI:10.1159/000315616] [PMID]
Type of Study: Original article |
Received: 2017/01/23 | Accepted: 2018/04/18 | Published: 2018/09/1
Received: 2017/01/23 | Accepted: 2018/04/18 | Published: 2018/09/1
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
