Fri, Apr 26, 2024
Volume 7, Issue 2 (6-2018)
2018, 7(2): 57-62 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Maleki L, Arzhang E, Alizadeh L. A Review of Signet Ring Cells in Salivary Gland Tumors. Journal title 2018; 7 (2) :57-62
URL: http://3dj.gums.ac.ir/article-1-310-en.html
URL: http://3dj.gums.ac.ir/article-1-310-en.html



1- Assistant Professor, Dental Research Center, Department of Oral and Maxillofacial Surgery, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Assistant Professor, Department of Oral and Maxillofacial Pathology, School of Dentistry, Shahrekord University of Medical Sciences, Shahrekord, Iran.
3- Assistant Professor, Dental Research Center, Department of Oral and Maxillofacial Pathology, School of Dentistry, Birjand University of Medical Sciences, Birjand, Iran. , alizadeh13642001@yahoo.com
2- Assistant Professor, Department of Oral and Maxillofacial Pathology, School of Dentistry, Shahrekord University of Medical Sciences, Shahrekord, Iran.
3- Assistant Professor, Dental Research Center, Department of Oral and Maxillofacial Pathology, School of Dentistry, Birjand University of Medical Sciences, Birjand, Iran. , alizadeh13642001@yahoo.com
Keywords: Signet Ring Cells, Salivary gland, Sublingual, Submandibular, Parotid, Salivary gland carcinoma
Full-Text [PDF 843 kb]
(937 Downloads)
Full-Text: (1104 Views)
1. Introduction
Signet Ring Cells (SRCs) are often present in gastrointestinal invasive carcinomas, the gallbladder, breast, and lungs. These cells have been seen in many lesions and other organs with a much smaller outbreak. SRCs are not always indicative of malignancy, as SRCs have been already seen in the microscopic samples obtained from the colon of patients suffering from colitis and in the bile ducts removed because of the stones [1].
Signet ring cell adenocarcinoma of the minor salivary glands was first introduced by Ghannoum and Freedman in 2004 [2]. Salivary gland tumors are an important group of head and neck tumors and 9% to 23% of primary salivary epithelial tumors are formed in the secondary salivary glands, 50% of which are malignant. Although SRC adenocarcinoma is a very rare subcutaneous salivary gland tumor, it includes 2% of the total malignancy of the secondary salivary glands.
The age range of the patients is 32-72 years and the female to male ratio is 2.5:1. Of course, the incidence of these tumors may be slightly higher, as some of them have been reported as Not Otherwise Specified (NOS) [3]. The most common site of minor salivary gland tumors is the hard palate and where the hard and soft palate meet [4]. They are also reported to be seen in different areas such as lips and buccal mucousa [5, 6]. These tumors are generally or typically seen as slowly growing asymptomatic masses, without invading the lower bone 4.
Histopathological features
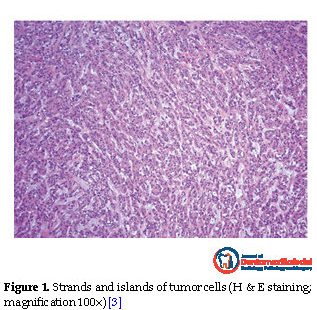
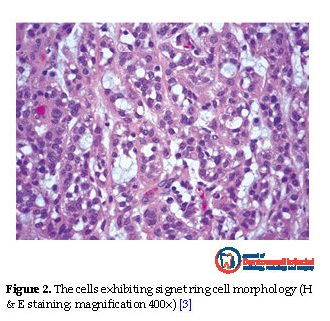
Signet ring cell carcinoma, is a non-capsular tumor with different growth patterns, from hypercellular regions with narrow parallel strands and anastomosing ribbons, consisting of ringed cells or possibly other mucin-secreting cells to hypocellular regions with scattered nests and small cells. They have microcystic centers, and regions with individual infiltrative cells of signet ring, or possibly other mucin-secreting cells, such as mucus and goblet cells, located in the extracellular mucin [4, 7, 8].
In fact, mucinous vacuoles within the cytoplasm may dilate the cell and create a foamy appearance, such as common mucous cells, or they may merge and squeeze the cell core against the plasma membrane, and create signet ring cells [7, 8] (Figure 1 and 2). Signet ring differentials like other areas of the body may occasionally be found in colloidal carcinomas of the salivary glands. However, tumors with more than 50% of colloidal constituents should be classified as colloid carcinoma. Also, a detailed search is required to eliminate the metastatic tumor 4.
Treatment and prognosis
A large surgical incision with tumor-free lining accompanied with lymphadenectomy for suspected lymph nodes or metastatic disease is a choice of treatment of this tumor.
2. Materials and Methods
In this review study, articles from 1984 to 2017 in the PubMed, Google Scholar were searched with the keywords of “Salivary gland carcinoma”, “parotid”, “submandibular”, “sublingual”, and “signet ring cells”. Eventually, 18 articles were found.
3. Results
Viewing SRCs in the salivary glands is not common. Although the signet ring cell adenocarcinoma has a low incidence, some of them may have been reported as NOS and in fact, it might have a higher incidence.
4. Discussion
The observation of SRCs in neoplasms and tumor-like lesions of the salivary glands is rare1. SRCs have been reported in benign tumors such as Warthin and malignant tumors, such as minor salivary gland adenocarcinomas and a mucin-rich subgroup of salivary duct carcinoma and in the carcinoma ex-pleomorphic adenoma [9-11]. In the case of the Warthin tumor, the presence of oncocytes along with SRCs is helpful in the final diagnosis [9].
Signet Ring Cells (SRCs) are often present in gastrointestinal invasive carcinomas, the gallbladder, breast, and lungs. These cells have been seen in many lesions and other organs with a much smaller outbreak. SRCs are not always indicative of malignancy, as SRCs have been already seen in the microscopic samples obtained from the colon of patients suffering from colitis and in the bile ducts removed because of the stones [1].
Signet ring cell adenocarcinoma of the minor salivary glands was first introduced by Ghannoum and Freedman in 2004 [2]. Salivary gland tumors are an important group of head and neck tumors and 9% to 23% of primary salivary epithelial tumors are formed in the secondary salivary glands, 50% of which are malignant. Although SRC adenocarcinoma is a very rare subcutaneous salivary gland tumor, it includes 2% of the total malignancy of the secondary salivary glands.
The age range of the patients is 32-72 years and the female to male ratio is 2.5:1. Of course, the incidence of these tumors may be slightly higher, as some of them have been reported as Not Otherwise Specified (NOS) [3]. The most common site of minor salivary gland tumors is the hard palate and where the hard and soft palate meet [4]. They are also reported to be seen in different areas such as lips and buccal mucousa [5, 6]. These tumors are generally or typically seen as slowly growing asymptomatic masses, without invading the lower bone 4.
Histopathological features
Signet ring cell carcinoma, is a non-capsular tumor with different growth patterns, from hypercellular regions with narrow parallel strands and anastomosing ribbons, consisting of ringed cells or possibly other mucin-secreting cells to hypocellular regions with scattered nests and small cells. They have microcystic centers, and regions with individual infiltrative cells of signet ring, or possibly other mucin-secreting cells, such as mucus and goblet cells, located in the extracellular mucin [4, 7, 8].
In fact, mucinous vacuoles within the cytoplasm may dilate the cell and create a foamy appearance, such as common mucous cells, or they may merge and squeeze the cell core against the plasma membrane, and create signet ring cells [7, 8] (Figure 1 and 2). Signet ring differentials like other areas of the body may occasionally be found in colloidal carcinomas of the salivary glands. However, tumors with more than 50% of colloidal constituents should be classified as colloid carcinoma. Also, a detailed search is required to eliminate the metastatic tumor 4.
Treatment and prognosis
A large surgical incision with tumor-free lining accompanied with lymphadenectomy for suspected lymph nodes or metastatic disease is a choice of treatment of this tumor.
2. Materials and Methods
In this review study, articles from 1984 to 2017 in the PubMed, Google Scholar were searched with the keywords of “Salivary gland carcinoma”, “parotid”, “submandibular”, “sublingual”, and “signet ring cells”. Eventually, 18 articles were found.
3. Results
Viewing SRCs in the salivary glands is not common. Although the signet ring cell adenocarcinoma has a low incidence, some of them may have been reported as NOS and in fact, it might have a higher incidence.
4. Discussion
The observation of SRCs in neoplasms and tumor-like lesions of the salivary glands is rare1. SRCs have been reported in benign tumors such as Warthin and malignant tumors, such as minor salivary gland adenocarcinomas and a mucin-rich subgroup of salivary duct carcinoma and in the carcinoma ex-pleomorphic adenoma [9-11]. In the case of the Warthin tumor, the presence of oncocytes along with SRCs is helpful in the final diagnosis [9].
The mucin-rich variant of the Salivary Duct Carcinoma (mSDC) is very rare, and so far only 8 cases have been reported, of which 5 have SRCs. In 3 of these 5 samples containing SRCs, mSDC was a malignant component in pleomorphic adenoma and as a carcinoma ex-pleomorphic adenoma. In all of these cases, the survival rate has been reported to be low and about 10 to 28 months [11]. Signet ring cell adenocarcinoma is a kind of mucin-secreting adenocarcinoma, which often appears in minor salivary glands as an exophytic mass attached to the underlying tissue. The mean age of the affected patients is 56.4 years and is more common in women. However, this tumor has also been seen in the major salivary glands, such as parotid gland [12, 13].
In some cases, reports have indicated the presence of SRCs in the absence of mucin pools or lakes containing mucin [2, 12, 14]. The tumor is non-capsular and infiltrative. In cases reported by Singh et al. and Ghannoum et al., SRCs have been seen as cords and sheets of malignant cells with minor pleomorphism in salivary gland tumors [2, 12]. One case of mucus-producing adenopapillary carcinoma has also been reported in the minor salivary gland cells of the palate, whose microscopic view indicated a papillary pattern along with a large number of SRCs and mucin-contents [5]. This tumor in microscopic view may be mistaken with mucoepidermoid carcinoma, where one should attend to the absence of epidermoid, intermediate, and clear cells and their differences with SRCs for differentiation [12].
SRCs in parotid other than mucin-secreting adenocarcinoma, have also been reported by Michal et al. in a rare case of oncocytic cystadenoma. In this case, numerous SRCs with bland morphology and oncocytic cells have been reported. In the microscopic view of this tumor, the sheets of the oncocytic cells are surrounded by myoepithelial cells, and most of the oncocytic cells contain large intracytoplasmic vacuoles (4-50 μm) and nuclei is located environmental and have appeared in the form of a signet ring cell. In this case, staining for musicarmin and cytokeratin was negative but staining for anti-mitochondrial antibody have been reported positive [13]. Rarely, signet ring lymphoma has also been seen in salivary glands, which is different from salivary gland tumors in terms of morphology and immunohistochemical profiles [12].
One recurrence of centroblastic and centrocytic nodular lymphoma has been reported in the salivary glands, which likens a signet ring cell lymphoma, and in ultrastructural studies, the cells contain empty vacuoles or residual membrane and myelinoid [15].
In salivary gland malignancies where SRCs are seen, certainly metastatic lesions from other organs should be checked by accurate clinical and radiological examinations and laboratory evaluations such as thyroglobulin, Cytokeratin (CK), Carcino Embryonic Antigen (CEA), Alpha Feto Protein (AFP) , Cancer Antigen (CA-125), and Carbohydrate Antigen (CA)19-9 tests [12].
In cases where SRCs are seen in the tumor and Smooth Muscle Actin (SMA) marker reported as positive, clear cell epithelial-myoepithelial carcinoma is considered in differential diagnosis. This diagnosis could be ruled out thanks to the specific morphology of the SRCs and the negativity of S100 [12]. Because of the morphology of the tumor and its mucin content, it may be mistaken with mucoepidermoid carcinoma, particularly its clear cell variant, mucinous adenocarcinoma, and Polymorphous Low-Grade Adenocarcinoma (PLGA), which can be distinguished from mucoepidermoid carcinoma and mucinous adenocarcinoma with due attention to the general cytomorphology and growth pattern. Mucinous adenocarcinoma is a rare malignant neoplasm composed of floating epithelial cells in basophilic mucin lakes, separated by fibrous septa.
The cells are single or form duct-like structures, dense cords, or cell clusters. These cells are polyhedral or cubic and have eosinophilic and occasionally clear cytoplasm [3]. In PLGA, evident cellular eosinophilic cytoplasm, oval/round, and bland nuclei, pagetoid pattern around the nerve and infiltrative pattern of Indian file (Single file) around the tumor can help to diagnose and differentiate properly [3].
The mucinous variant of myoepithelioma is also a myoepithelial tumor with clear prominent cytoplasmic areas that often contain mucin content with the morphology of signet ring [16]. Unlike signet ring carcinomas in other organs, this tumor in the salivary glands is often referred to as low-grade neoplasm, where its recurrence and metastasis are rare after complete excision [12]. The subtype of the "signet ring" in gastric and esophageal adenocarcinoma is invasive and metastatic with poor prognosis [17]. However, in rare cases where metastases to the lymph node exist, besides complete excision, neck dissection and radiotherapy are also needed [18].
In the sample reported by Horn et al. a signet ring cell adenocarcinoma was found in the parotid gland that unlike the minor salivary glands, its metastasis was seen to the lymph node and brain [14]. The Ki67 index is the most useful immunohistochemical marker for determining the prognosis of patients with salivary gland tumors. In the case of high Ki67, the prognosis is poor and the survival rate is often low [19].
5. Conclusion
Signet ring cell adenocarcinoma of the salivary gland is rare and must be differentially diagnosed with more common tumors of the salivary glands such as mucoepidermoid carcinoma and PLGA. Although the features and prognosis of signet ring cell adenocarcinoma are known in other parts of the body such as the gastrointestinal tract, further studies and investigations are required to determine the exact prevalence of salivary gland signet ring adenocarcinoma, its features, prognosis, and treatment methods.
Paraffin blocks of the samples labeled as NOS adenocarcinoma should also be investigated in this regard because some of the signet ring cell adenocarcinomas of the salivary glands have been inappropriately reported as adenocarcinomas NOS.
Ethical Considerations
Compliance with ethical guidelines
There is no ethical principle to be considered doing this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Laleh Maleki: Study concept, study design, literature review, manuscript preparation; literature review, manuscript preparation: Elha Arzhang and Leili Alizadeh; and editing and review: Leili Alizadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors wish to give special thanks to Mohammad Alizadeh for his contributions to the manuscript.
References
Foschini MP, Baldovini C, Pennesi MG, Cocchi R, Simpson RH. Signetring celltumor of the minor salivary gland exhibiting benign behavior. Human Pathology. 2012; 43(2):303-6. [DOI:10.1016/j.humpath.2011.04.025]
Ghannoum JE, Freedman PD. Signet-ring cell (mucin-producing) adenocarcinomas of minor salivary glands. The American Journal of Surgical Pathology. 2004; 28(1):89-93. [DOI:10.1097/00000478-200401000-00010] [PMID]
Bastaki J, Summersgill K. Signet-ring cell (mucin-producing) adenocarcinoma of minor salivary glands: Report of a case. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology. 2010; 110(4):e33-6. [DOI:10.1016/j.tripleo.2010.05.066]
Gneep D. Diagnostic surgical pathology of the head & neck. 2nd Edition. Philadelphia: Saunders Elsevier; 2009. [DOI:10.1016/B978-1-4160-2589-4.00006-1]
deAraújo VC, de Sousa SO, Lopes EA, de Araújo NS, Sesso A. Mucus producing adenopapillary carcinoma of minor salivary gland origin with signet ring cells and intracytoplasmiclumina. A light and electron microscopic study. International Archives of Otorhinolaryngology. 1988; 245(3):145-50. [DOI:10.1007/BF00464016]
Zamecnik M, Gogora M. Signet-ring cells simulating carcinoma in minor salivary gland of the lip. Pathology-Research and Practice. 1999; 195(10):723-4. [DOI:10.1016/S0344-0338(99)80068-5]
Kumar V, Abbas A, Fausto N. [Pathologic basis of disease (Persian)]. 7th Edition. Philadelphia: Elsevier Saunders; 2005.
Dyhimi P. Pathologic of salivary gland. 1st edition. Isfahan: Isfahan University of Medical Sciences; 2015.
Bellevicine C, Iaccarino A, Malapelle U, Troncone G. Warthin tumor with signet-ring cell features as a pitfall in salivary gland cytopathology. Acta Cytologica. 2013; 57(3):309-12. [DOI:10.1159/000348248]
Bastaki JM, Purgina BM, Dacic S, Seethala RR. Primary signet-ring cell (mucin-producing) adenocarcinoma of minor salivary glands: A clinicopathologic, immunohistochemical and molecular survey. Laboratory Investigation. 2012; 92:304A-305A.
Kusafuka K, Maeda M, Honda M, Nakajima T. Mucin-rich salivary duct carcinoma with signet-ring cell feature ex pleomorphic adenoma of the submandibular gland: A case report of an unusual histology with immunohistochemical analysis and review of the literature. Medical Molecular Morphology. 2012; 45(1):45-52. [DOI:10.1007/s00795-011-0554-3]
Singh M, Khurana N, Wadhwa R, Gulati A. Signet ring carcinoma parotid gland: A case report. Head & Neck. 2011; 33(11):1656-9. [DOI:10.1002/hed.21435]
Michal M, Hrabal P, Skálová A. Oncocyticcystadenoma of the parotid gland with prominent signet-ring cell features. International Journal of Surgical Pathology. 1998; 48(8):629-33. [DOI:10.1111/j.1440-1827.1998.tb03961.x] [PMID]
Horn KD, Richert CA, Rajan PB, Bastacky SI, Peterson AB, Barnes EL. Cytological findings of metastatic mucin secreting adenocarcinoma of brain from parotid gland primary. Cytopathology. 1999; 10(5):341-4. [DOI:10.1046/j.1365-2303.1999.00163.x] [PMID]
Stramignoni A, Palestro G, Coda R, Micca FB, Stramignoni D. Signet ring cell lymphoma in salivary gland. An immunohistochemical and ultrastructural study. Applied Immunohistochemistry & Molecular Morphology. 1984; 2(2):76-84. [PMID]
Skálová A, Gnepp DR, Lewis JS Jr, Hunt JL, Bishop JA, Hellquist H, et al. Newly described entities in salivary gland pathology. The American Journal of Surgical Pathology. 2017; 41(8):e33-e47. [DOI:10.1097/PAS.0000000000000883]
Carrott P. Signet rings around the world. Seminars in Thoracic and Cardiovascular Surgery. 2017; 29(1):118. [DOI:10.1053/j.semtcvs.2017.03.004]
Veit JA, Reichelt U, Tesche S. Signet ring cell adenocarcinoma of the oropharynx: Presentation of a rare case and review of the literature. Auris Nasus Larynx. 2009; 36(6):717-20. [DOI:10.1016/j.anl.2009.01.013]
Cheuk W, Chan JK. Advances in salivary gland pathology. Histopathology. 2007; 51(1):1-20. [DOI:10.1111/j.1365-2559.2007.02719.x] [PMID]
In some cases, reports have indicated the presence of SRCs in the absence of mucin pools or lakes containing mucin [2, 12, 14]. The tumor is non-capsular and infiltrative. In cases reported by Singh et al. and Ghannoum et al., SRCs have been seen as cords and sheets of malignant cells with minor pleomorphism in salivary gland tumors [2, 12]. One case of mucus-producing adenopapillary carcinoma has also been reported in the minor salivary gland cells of the palate, whose microscopic view indicated a papillary pattern along with a large number of SRCs and mucin-contents [5]. This tumor in microscopic view may be mistaken with mucoepidermoid carcinoma, where one should attend to the absence of epidermoid, intermediate, and clear cells and their differences with SRCs for differentiation [12].
SRCs in parotid other than mucin-secreting adenocarcinoma, have also been reported by Michal et al. in a rare case of oncocytic cystadenoma. In this case, numerous SRCs with bland morphology and oncocytic cells have been reported. In the microscopic view of this tumor, the sheets of the oncocytic cells are surrounded by myoepithelial cells, and most of the oncocytic cells contain large intracytoplasmic vacuoles (4-50 μm) and nuclei is located environmental and have appeared in the form of a signet ring cell. In this case, staining for musicarmin and cytokeratin was negative but staining for anti-mitochondrial antibody have been reported positive [13]. Rarely, signet ring lymphoma has also been seen in salivary glands, which is different from salivary gland tumors in terms of morphology and immunohistochemical profiles [12].
One recurrence of centroblastic and centrocytic nodular lymphoma has been reported in the salivary glands, which likens a signet ring cell lymphoma, and in ultrastructural studies, the cells contain empty vacuoles or residual membrane and myelinoid [15].
In salivary gland malignancies where SRCs are seen, certainly metastatic lesions from other organs should be checked by accurate clinical and radiological examinations and laboratory evaluations such as thyroglobulin, Cytokeratin (CK), Carcino Embryonic Antigen (CEA), Alpha Feto Protein (AFP) , Cancer Antigen (CA-125), and Carbohydrate Antigen (CA)19-9 tests [12].
In cases where SRCs are seen in the tumor and Smooth Muscle Actin (SMA) marker reported as positive, clear cell epithelial-myoepithelial carcinoma is considered in differential diagnosis. This diagnosis could be ruled out thanks to the specific morphology of the SRCs and the negativity of S100 [12]. Because of the morphology of the tumor and its mucin content, it may be mistaken with mucoepidermoid carcinoma, particularly its clear cell variant, mucinous adenocarcinoma, and Polymorphous Low-Grade Adenocarcinoma (PLGA), which can be distinguished from mucoepidermoid carcinoma and mucinous adenocarcinoma with due attention to the general cytomorphology and growth pattern. Mucinous adenocarcinoma is a rare malignant neoplasm composed of floating epithelial cells in basophilic mucin lakes, separated by fibrous septa.
The cells are single or form duct-like structures, dense cords, or cell clusters. These cells are polyhedral or cubic and have eosinophilic and occasionally clear cytoplasm [3]. In PLGA, evident cellular eosinophilic cytoplasm, oval/round, and bland nuclei, pagetoid pattern around the nerve and infiltrative pattern of Indian file (Single file) around the tumor can help to diagnose and differentiate properly [3].
The mucinous variant of myoepithelioma is also a myoepithelial tumor with clear prominent cytoplasmic areas that often contain mucin content with the morphology of signet ring [16]. Unlike signet ring carcinomas in other organs, this tumor in the salivary glands is often referred to as low-grade neoplasm, where its recurrence and metastasis are rare after complete excision [12]. The subtype of the "signet ring" in gastric and esophageal adenocarcinoma is invasive and metastatic with poor prognosis [17]. However, in rare cases where metastases to the lymph node exist, besides complete excision, neck dissection and radiotherapy are also needed [18].
In the sample reported by Horn et al. a signet ring cell adenocarcinoma was found in the parotid gland that unlike the minor salivary glands, its metastasis was seen to the lymph node and brain [14]. The Ki67 index is the most useful immunohistochemical marker for determining the prognosis of patients with salivary gland tumors. In the case of high Ki67, the prognosis is poor and the survival rate is often low [19].
5. Conclusion
Signet ring cell adenocarcinoma of the salivary gland is rare and must be differentially diagnosed with more common tumors of the salivary glands such as mucoepidermoid carcinoma and PLGA. Although the features and prognosis of signet ring cell adenocarcinoma are known in other parts of the body such as the gastrointestinal tract, further studies and investigations are required to determine the exact prevalence of salivary gland signet ring adenocarcinoma, its features, prognosis, and treatment methods.
Paraffin blocks of the samples labeled as NOS adenocarcinoma should also be investigated in this regard because some of the signet ring cell adenocarcinomas of the salivary glands have been inappropriately reported as adenocarcinomas NOS.
Ethical Considerations
Compliance with ethical guidelines
There is no ethical principle to be considered doing this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Laleh Maleki: Study concept, study design, literature review, manuscript preparation; literature review, manuscript preparation: Elha Arzhang and Leili Alizadeh; and editing and review: Leili Alizadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors wish to give special thanks to Mohammad Alizadeh for his contributions to the manuscript.
References
Foschini MP, Baldovini C, Pennesi MG, Cocchi R, Simpson RH. Signetring celltumor of the minor salivary gland exhibiting benign behavior. Human Pathology. 2012; 43(2):303-6. [DOI:10.1016/j.humpath.2011.04.025]
Ghannoum JE, Freedman PD. Signet-ring cell (mucin-producing) adenocarcinomas of minor salivary glands. The American Journal of Surgical Pathology. 2004; 28(1):89-93. [DOI:10.1097/00000478-200401000-00010] [PMID]
Bastaki J, Summersgill K. Signet-ring cell (mucin-producing) adenocarcinoma of minor salivary glands: Report of a case. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology. 2010; 110(4):e33-6. [DOI:10.1016/j.tripleo.2010.05.066]
Gneep D. Diagnostic surgical pathology of the head & neck. 2nd Edition. Philadelphia: Saunders Elsevier; 2009. [DOI:10.1016/B978-1-4160-2589-4.00006-1]
deAraújo VC, de Sousa SO, Lopes EA, de Araújo NS, Sesso A. Mucus producing adenopapillary carcinoma of minor salivary gland origin with signet ring cells and intracytoplasmiclumina. A light and electron microscopic study. International Archives of Otorhinolaryngology. 1988; 245(3):145-50. [DOI:10.1007/BF00464016]
Zamecnik M, Gogora M. Signet-ring cells simulating carcinoma in minor salivary gland of the lip. Pathology-Research and Practice. 1999; 195(10):723-4. [DOI:10.1016/S0344-0338(99)80068-5]
Kumar V, Abbas A, Fausto N. [Pathologic basis of disease (Persian)]. 7th Edition. Philadelphia: Elsevier Saunders; 2005.
Dyhimi P. Pathologic of salivary gland. 1st edition. Isfahan: Isfahan University of Medical Sciences; 2015.
Bellevicine C, Iaccarino A, Malapelle U, Troncone G. Warthin tumor with signet-ring cell features as a pitfall in salivary gland cytopathology. Acta Cytologica. 2013; 57(3):309-12. [DOI:10.1159/000348248]
Bastaki JM, Purgina BM, Dacic S, Seethala RR. Primary signet-ring cell (mucin-producing) adenocarcinoma of minor salivary glands: A clinicopathologic, immunohistochemical and molecular survey. Laboratory Investigation. 2012; 92:304A-305A.
Kusafuka K, Maeda M, Honda M, Nakajima T. Mucin-rich salivary duct carcinoma with signet-ring cell feature ex pleomorphic adenoma of the submandibular gland: A case report of an unusual histology with immunohistochemical analysis and review of the literature. Medical Molecular Morphology. 2012; 45(1):45-52. [DOI:10.1007/s00795-011-0554-3]
Singh M, Khurana N, Wadhwa R, Gulati A. Signet ring carcinoma parotid gland: A case report. Head & Neck. 2011; 33(11):1656-9. [DOI:10.1002/hed.21435]
Michal M, Hrabal P, Skálová A. Oncocyticcystadenoma of the parotid gland with prominent signet-ring cell features. International Journal of Surgical Pathology. 1998; 48(8):629-33. [DOI:10.1111/j.1440-1827.1998.tb03961.x] [PMID]
Horn KD, Richert CA, Rajan PB, Bastacky SI, Peterson AB, Barnes EL. Cytological findings of metastatic mucin secreting adenocarcinoma of brain from parotid gland primary. Cytopathology. 1999; 10(5):341-4. [DOI:10.1046/j.1365-2303.1999.00163.x] [PMID]
Stramignoni A, Palestro G, Coda R, Micca FB, Stramignoni D. Signet ring cell lymphoma in salivary gland. An immunohistochemical and ultrastructural study. Applied Immunohistochemistry & Molecular Morphology. 1984; 2(2):76-84. [PMID]
Skálová A, Gnepp DR, Lewis JS Jr, Hunt JL, Bishop JA, Hellquist H, et al. Newly described entities in salivary gland pathology. The American Journal of Surgical Pathology. 2017; 41(8):e33-e47. [DOI:10.1097/PAS.0000000000000883]
Carrott P. Signet rings around the world. Seminars in Thoracic and Cardiovascular Surgery. 2017; 29(1):118. [DOI:10.1053/j.semtcvs.2017.03.004]
Veit JA, Reichelt U, Tesche S. Signet ring cell adenocarcinoma of the oropharynx: Presentation of a rare case and review of the literature. Auris Nasus Larynx. 2009; 36(6):717-20. [DOI:10.1016/j.anl.2009.01.013]
Cheuk W, Chan JK. Advances in salivary gland pathology. Histopathology. 2007; 51(1):1-20. [DOI:10.1111/j.1365-2559.2007.02719.x] [PMID]
Received: 2017/12/17 | Accepted: 2018/04/2 | Published: 2018/06/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
