Mon, Feb 2, 2026
Volume 7, Issue 1 (3-2018)
2018, 7(1): 29-36 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Basirat M, Kia S J, Motevasseli S, Dadgaran I. Knowledge and Attitude of Faculty Members Towards Integrated Curriculum in Dentistry and Its Related Factors. Journal title 2018; 7 (1) :29-36
URL: http://3dj.gums.ac.ir/article-1-309-en.html
URL: http://3dj.gums.ac.ir/article-1-309-en.html



1- Assistant Professor, Medical Education Research Center, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Oral and Maxillofacial Medicine, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
3- Assistant Professor, Department of Oral and Maxillofacial Medicine, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Medical Education Research Center, Guilan University of Medical Sciences, Rasht, Iran. ,i_dadgaran@yahoo.com
2- Department of Oral and Maxillofacial Medicine, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
3- Assistant Professor, Department of Oral and Maxillofacial Medicine, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Medical Education Research Center, Guilan University of Medical Sciences, Rasht, Iran. ,
Full-Text [PDF 745 kb]
(1593 Downloads)
| Abstract (HTML) (3336 Views)
Faculty members’ Mean±SD score in knowledge was 3.2±0.273. Four (7.8%) faculty members presented high levels of knowledge, 14 (27.5%) good levels of knowledge and 22 (43.1%) moderate levels of knowledge. A total of 11 (21.6%) members did not complete the integration knowledge part. Table 2 presents the faculty members’ answers to questions about knowledge towards integrated curriculum in dentistry.



Regarding the disadvantages of integration plan, faculty members' reluctance for proper interaction can result in incomplete coverage of content and basic principles of a discipline and unwanted removal of some topics. In addition, professors should master modern teaching methods. However, integration of curriculum is a costly program, and integrated education can have adverse effects on the process of choosing specialty fields and occupation by the students [5, 8] as it is consistent with our study findings. The faculty members' main positive opinions included coordination between professors, school authorities’ support of integration of curriculum, and adherence to curriculum for teaching lessons. In the study conducted by Hassanzadeh and Nasiri, the students’ attitudes and opinions on team-based learning and presentation of integrated pharmacology courses was positive [15].
There was not any significant relationship between knowledge and the attitude scores with work experience in the present study. It was probably due to the fact that there was not any significant relationship between these scores and their age. There was not any significant statistical relationship between knowledge and also attitude of faculty members and their participation in workshop or journal clubs of integration, curriculum, and evaluation of students. This was probably due to the fact that most of them didn’t participate in these workshops.
5. Conclusion
Based on the results of the present study, dentistry faculty members’ knowledge about curriculum integration was moderate. About 65% of the faculty members had negative attitude about integrated curriculum. There were not significant relationships between age, gender and work experience with knowledge and also attitude scores. Given the need for change in teaching methods, we hope that by preparation of integration curriculum requirements and its implementation, the student’s problem-solving skills increases and they gain deep sustainable knowledge. It is suggested that similar qualitative studies be conducted at other dental schools of Iran in order to promote dentistry education level of Iran by identification of obstacles to implement of this project.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval code of the present study is IR.GUMS.REC.1394.
Funding
This research was granted by Research Foundation of Guilan University of Medical Sciences in 2016.
Authors contributions
Responsible for the study concept and design, acquisition of data, drafting, and critical revision for important intellectual content: Maryam Basirat and Ideh dadgaran; Responsible for the administrative, technical, and material support as well as the study supervision: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We would like to thank the Vice Chancellor of Research Foundation for financial support. In addition, The authors would like to thank Dr Mohammad Ghaffari for performing statistical analysis and Sana Alavi Nikoo in conducting a literature review and distribution of questionnaire.
References
Full-Text: (3665 Views)
1. Introduction
The term ‘Integration’ refers to creation of an integrated system by combining separate components [1]. Various studies on knowledge acquisition have pointed out to limited or inadequate time to teach a subject due to the large number of curricula, mismatch of educational content with practical application, and overlooking learning qualities in natural settings as reasons for necessity of curriculum integration. An integrated curriculum prevents repetition of unnecessary content details compared to problem-based programs, and it can produce high-level intellectual skills [2, 3].
Creation of unity and interdisciplinary relationship, higher student motivation, provision of more effective education (content retention), achievement of higher educational goals (problem solving skills and its application), increase in communication and collaboration between professors, and rationalization of educational resources are among the advantages of integration plan [2, 4, 5]. This approach can even increase learners’ motivation, self-esteem, positive attitude, and learning ability [6]. In other words, in an integrated system, the students experience a disease-based approach instead of a patient-based approach [5, 7]. On the other hand, possibility of not covering all content and basic principles of any discipline, unwanted removal of some subjects due to neglect, teachers’ higher mastery in traditional approaches, high cost of integrated education, and existence of adverse effects in guiding students in choosing future jobs and career are among the disadvantages of integration [4, 5].
There are two types of integration in medical education: horizontal and vertical [5]. To reach an integrated curriculum stage from a subject-based curriculum, we should pass 11 consecutive stages in which the subject-based planning is performed in the first four stages (isolation, awareness, synchronization, and nesting). The next six stages (temporal co-ordination, sharing, correlation, complementary program, multidiscipline program, and interdisciplinary curriculum) emphasis on multidisciplinary integration. The integration is fully accomplished in the final stage i.e. transdiscipline, which does not focus on learning a topic or subject, but exemplifying the real world [5, 8, 9].
Integration of curriculum is currently performing at dental schools. The integration is affected by many factors such as proper and purposive planning, optimal conditions and facilities, and especially teachers’ experience and attitude on the context [1, 2, 8, 10]. Although teachers often accept and agree with integration, some disagreement is also observed at some stages of integration, and smooth transition of integration stages depends on proper and purposive planning, teachers’ experience and positive attitude, and existence of optimal conditions and facilities at dental schools [4, 6, 8]. Therefore, this research aimed to investigate knowledge and attitude of dentistry faculty members about integrated curriculum and its related factors.
2. Materials and Methods
This descriptive cross-sectional study was conducted on 51 (out of total 74) faculty members in Dental School, Guilan University of Medical Sciences. Membership in Guilan Dental School was the inclusion criterion, but faculty member’s incomplete questionnaire was the exclusion criterion.
The study data collection tool was a researcher-made questionnaire consisting of three parts; demographic characteristics, knowledge, and attitude. Knowledge and attitude parts were consisted of 8 and 18 questions, respectively. In knowledge part, wrong answer to each question scores 0 and the right answer 1. The total knowledge scores were classified as follows: excellent (6-8), good (4-5), moderate (2-3), and weak (0-1). In calculation of attitude score, score of 5 was given to complete agreement, 4 to agreement, 3 to no opinion, 2 to disagreement, and 1 to complete disagreement. In another method of calculation, the subjects with scores <50% were put in the negative attitude group, and those with scores >50% were put in the positive attitude group [11].
Validity of the questionnaire was assessed through content validity (CVI=0.8, CVR=0.86) and its reliability was checked through test-retest (r=0.8). The questionnaires were completed through distant way by professors in Dental School of Guilan University of Medical Sciences, and they were collected a week after distribution. The obtained data were analyzed by using descriptive statistics, and inferential statistics of the Independent t-test, and Mann-Whitney U, Pearson correlation, and Spearman rank tests in SPSS (version 20).
3. Results
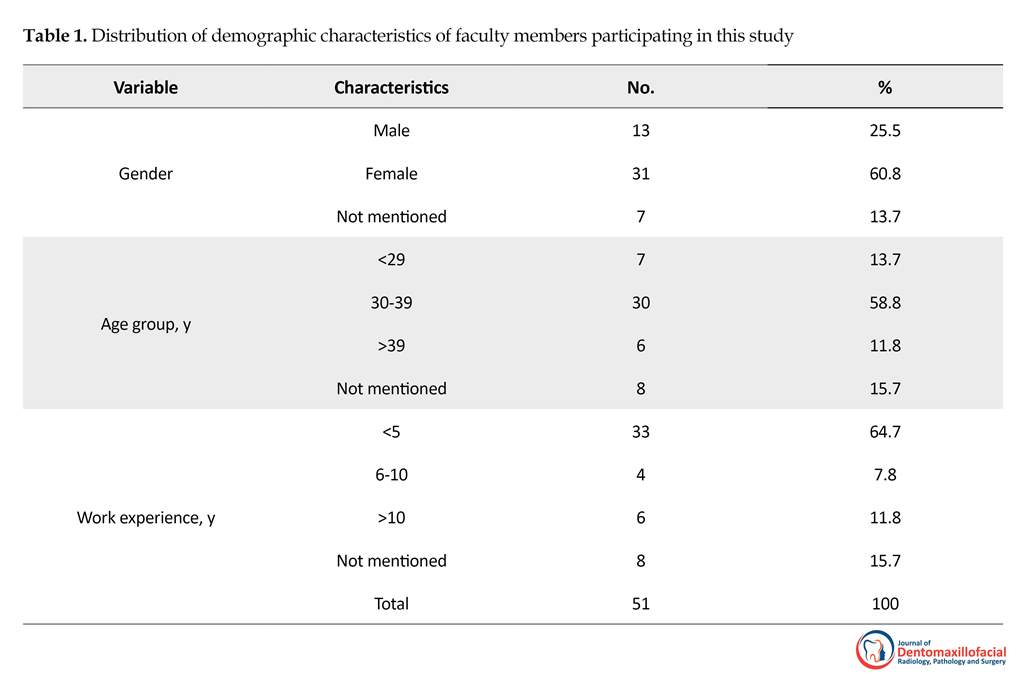
Out of 74 faculty members, 51 people participated in the present study. Mean±SD age of the subjects was 34.35±1.009 years (range: 27-54 y) and subjects’ Mean±SD work experience was 4.49±0.877 years (range: 1-24 y). Table 1 presents distribution of demographic characteristics of faculty members. A total of 33 subjects (64.7%) had not attended any workshop or journal club of integrated curriculum, also 44 subjects (86.3%) had not attended any workshop or journal club of evaluations.
The term ‘Integration’ refers to creation of an integrated system by combining separate components [1]. Various studies on knowledge acquisition have pointed out to limited or inadequate time to teach a subject due to the large number of curricula, mismatch of educational content with practical application, and overlooking learning qualities in natural settings as reasons for necessity of curriculum integration. An integrated curriculum prevents repetition of unnecessary content details compared to problem-based programs, and it can produce high-level intellectual skills [2, 3].
Creation of unity and interdisciplinary relationship, higher student motivation, provision of more effective education (content retention), achievement of higher educational goals (problem solving skills and its application), increase in communication and collaboration between professors, and rationalization of educational resources are among the advantages of integration plan [2, 4, 5]. This approach can even increase learners’ motivation, self-esteem, positive attitude, and learning ability [6]. In other words, in an integrated system, the students experience a disease-based approach instead of a patient-based approach [5, 7]. On the other hand, possibility of not covering all content and basic principles of any discipline, unwanted removal of some subjects due to neglect, teachers’ higher mastery in traditional approaches, high cost of integrated education, and existence of adverse effects in guiding students in choosing future jobs and career are among the disadvantages of integration [4, 5].
There are two types of integration in medical education: horizontal and vertical [5]. To reach an integrated curriculum stage from a subject-based curriculum, we should pass 11 consecutive stages in which the subject-based planning is performed in the first four stages (isolation, awareness, synchronization, and nesting). The next six stages (temporal co-ordination, sharing, correlation, complementary program, multidiscipline program, and interdisciplinary curriculum) emphasis on multidisciplinary integration. The integration is fully accomplished in the final stage i.e. transdiscipline, which does not focus on learning a topic or subject, but exemplifying the real world [5, 8, 9].
Integration of curriculum is currently performing at dental schools. The integration is affected by many factors such as proper and purposive planning, optimal conditions and facilities, and especially teachers’ experience and attitude on the context [1, 2, 8, 10]. Although teachers often accept and agree with integration, some disagreement is also observed at some stages of integration, and smooth transition of integration stages depends on proper and purposive planning, teachers’ experience and positive attitude, and existence of optimal conditions and facilities at dental schools [4, 6, 8]. Therefore, this research aimed to investigate knowledge and attitude of dentistry faculty members about integrated curriculum and its related factors.
2. Materials and Methods
This descriptive cross-sectional study was conducted on 51 (out of total 74) faculty members in Dental School, Guilan University of Medical Sciences. Membership in Guilan Dental School was the inclusion criterion, but faculty member’s incomplete questionnaire was the exclusion criterion.
The study data collection tool was a researcher-made questionnaire consisting of three parts; demographic characteristics, knowledge, and attitude. Knowledge and attitude parts were consisted of 8 and 18 questions, respectively. In knowledge part, wrong answer to each question scores 0 and the right answer 1. The total knowledge scores were classified as follows: excellent (6-8), good (4-5), moderate (2-3), and weak (0-1). In calculation of attitude score, score of 5 was given to complete agreement, 4 to agreement, 3 to no opinion, 2 to disagreement, and 1 to complete disagreement. In another method of calculation, the subjects with scores <50% were put in the negative attitude group, and those with scores >50% were put in the positive attitude group [11].
Validity of the questionnaire was assessed through content validity (CVI=0.8, CVR=0.86) and its reliability was checked through test-retest (r=0.8). The questionnaires were completed through distant way by professors in Dental School of Guilan University of Medical Sciences, and they were collected a week after distribution. The obtained data were analyzed by using descriptive statistics, and inferential statistics of the Independent t-test, and Mann-Whitney U, Pearson correlation, and Spearman rank tests in SPSS (version 20).
3. Results
Out of 74 faculty members, 51 people participated in the present study. Mean±SD age of the subjects was 34.35±1.009 years (range: 27-54 y) and subjects’ Mean±SD work experience was 4.49±0.877 years (range: 1-24 y). Table 1 presents distribution of demographic characteristics of faculty members. A total of 33 subjects (64.7%) had not attended any workshop or journal club of integrated curriculum, also 44 subjects (86.3%) had not attended any workshop or journal club of evaluations.
Faculty members’ Mean±SD score in knowledge was 3.2±0.273. Four (7.8%) faculty members presented high levels of knowledge, 14 (27.5%) good levels of knowledge and 22 (43.1%) moderate levels of knowledge. A total of 11 (21.6%) members did not complete the integration knowledge part. Table 2 presents the faculty members’ answers to questions about knowledge towards integrated curriculum in dentistry.
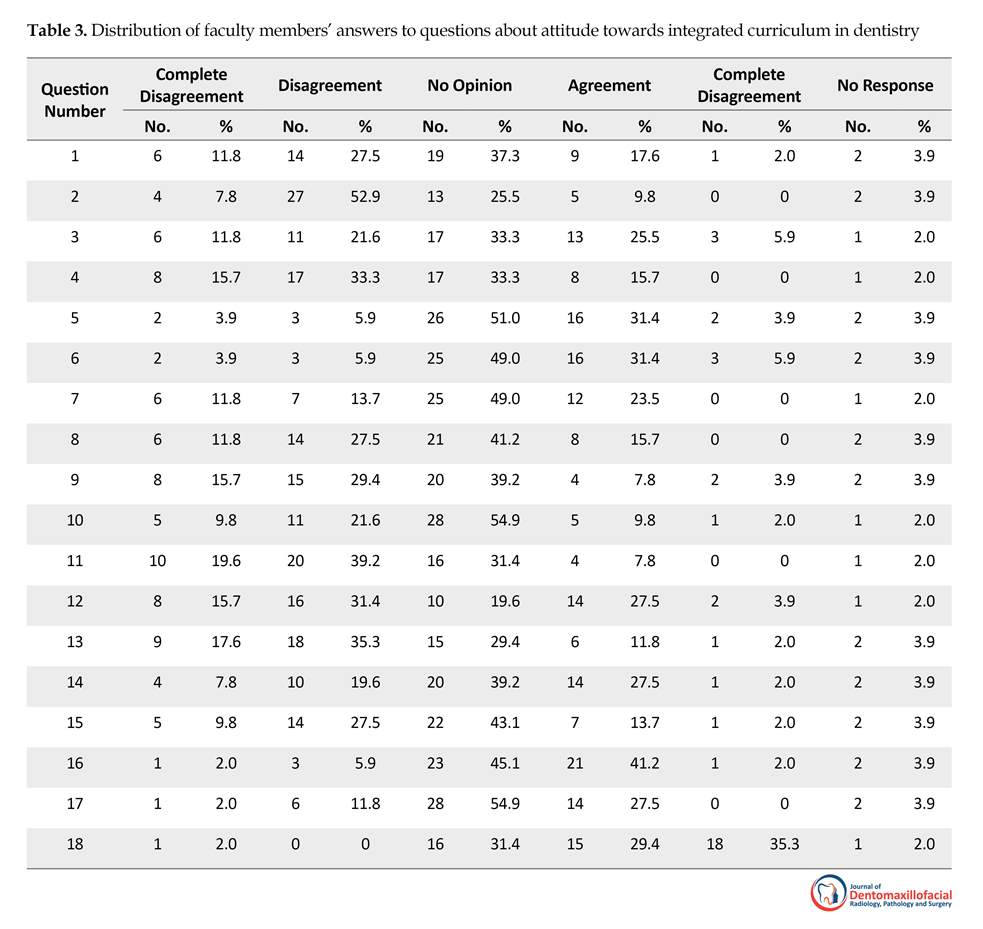
A total of 33 (64.7%) faculty members had negative attitude, but 14 (27.5%) members had positive attitude towards integration plan, and 4 (7.8%) members did not complete the attitude questions. In total, 1 (2%) faculty member had complete disagreement attitude, 11 (21.6%) members had disagreement attitude, 5 (9.8%) members had agreement attitude, 30 (58.8%) were without any opinion, and 4 (7.8%) members did not express their attitude. Table 3 presents faculty members’ answers to questions about attitude towards integrated curriculum in dentistry.
There were not any significant relationships between age and knowledge scores based on Pearson correlation test (P=0.990), between gender and knowledge scores using Independent t-test (P=0.923), and between work experience and knowledge scores using Spearman correlation test (P=0.684).
There were not any significant relationships between age and attitude scores using Spearman correlation test (P=0.547), between gender and attitude scores by Mann-Whitney U test (P=0.822), and between work experience and attitude scores based on Spearman correlation test (P=0.077). According to studied regression of predictive variables on knowledge score (Table 4) and also attitude scores (Table 5), none of variables of age, gender, and work experience or participation in workshops or journal clubs of integration, curriculum, and evaluation of student had any significant effects on these scores.
There were not any significant relationships between age and knowledge scores based on Pearson correlation test (P=0.990), between gender and knowledge scores using Independent t-test (P=0.923), and between work experience and knowledge scores using Spearman correlation test (P=0.684).
There were not any significant relationships between age and attitude scores using Spearman correlation test (P=0.547), between gender and attitude scores by Mann-Whitney U test (P=0.822), and between work experience and attitude scores based on Spearman correlation test (P=0.077). According to studied regression of predictive variables on knowledge score (Table 4) and also attitude scores (Table 5), none of variables of age, gender, and work experience or participation in workshops or journal clubs of integration, curriculum, and evaluation of student had any significant effects on these scores.
4. Discussion
The necessity of change in teaching system and its integration has been emphasized by the American Society for Medical Education in 1982 and by the English Society for Medical Education in 1993 and 1994 [5, 8]. It has already been implemented in many countries [10-14], and recommended in our country, too.
Results of this study indicated that knowledge of dentistry faculty members about integration in education system was moderate. In the present study, basic concepts of knowledge were studied. This problem can be due to the non-participation of many faculty members in integration workshops or journal clubs, low work experience, a little time after performance of integration plan, and the lack of experience in this field in addition to structural problems [9]. However, taxonomy of questions also has a great impact on knowledge score. According to conducted studies, this study is one of the few studies which investigate dental professors’ knowledge and attitudes about integration in dentistry curriculum.
A total of 33 (64.7%) faculty members had negative attitude toward curriculum integration. In the present study, the main reasons for faculty members’ disagreement with integration of curriculum were their unawareness about it, lack of evaluation programs within departments, inappropriate planning and facilities, and educational experts’ unawareness of curriculum integration which are the requirements of this process.
The necessity of change in teaching system and its integration has been emphasized by the American Society for Medical Education in 1982 and by the English Society for Medical Education in 1993 and 1994 [5, 8]. It has already been implemented in many countries [10-14], and recommended in our country, too.
Results of this study indicated that knowledge of dentistry faculty members about integration in education system was moderate. In the present study, basic concepts of knowledge were studied. This problem can be due to the non-participation of many faculty members in integration workshops or journal clubs, low work experience, a little time after performance of integration plan, and the lack of experience in this field in addition to structural problems [9]. However, taxonomy of questions also has a great impact on knowledge score. According to conducted studies, this study is one of the few studies which investigate dental professors’ knowledge and attitudes about integration in dentistry curriculum.
A total of 33 (64.7%) faculty members had negative attitude toward curriculum integration. In the present study, the main reasons for faculty members’ disagreement with integration of curriculum were their unawareness about it, lack of evaluation programs within departments, inappropriate planning and facilities, and educational experts’ unawareness of curriculum integration which are the requirements of this process.
Regarding the disadvantages of integration plan, faculty members' reluctance for proper interaction can result in incomplete coverage of content and basic principles of a discipline and unwanted removal of some topics. In addition, professors should master modern teaching methods. However, integration of curriculum is a costly program, and integrated education can have adverse effects on the process of choosing specialty fields and occupation by the students [5, 8] as it is consistent with our study findings. The faculty members' main positive opinions included coordination between professors, school authorities’ support of integration of curriculum, and adherence to curriculum for teaching lessons. In the study conducted by Hassanzadeh and Nasiri, the students’ attitudes and opinions on team-based learning and presentation of integrated pharmacology courses was positive [15].
There was not any significant relationship between knowledge and the attitude scores with work experience in the present study. It was probably due to the fact that there was not any significant relationship between these scores and their age. There was not any significant statistical relationship between knowledge and also attitude of faculty members and their participation in workshop or journal clubs of integration, curriculum, and evaluation of students. This was probably due to the fact that most of them didn’t participate in these workshops.
5. Conclusion
Based on the results of the present study, dentistry faculty members’ knowledge about curriculum integration was moderate. About 65% of the faculty members had negative attitude about integrated curriculum. There were not significant relationships between age, gender and work experience with knowledge and also attitude scores. Given the need for change in teaching methods, we hope that by preparation of integration curriculum requirements and its implementation, the student’s problem-solving skills increases and they gain deep sustainable knowledge. It is suggested that similar qualitative studies be conducted at other dental schools of Iran in order to promote dentistry education level of Iran by identification of obstacles to implement of this project.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval code of the present study is IR.GUMS.REC.1394.
Funding
This research was granted by Research Foundation of Guilan University of Medical Sciences in 2016.
Authors contributions
Responsible for the study concept and design, acquisition of data, drafting, and critical revision for important intellectual content: Maryam Basirat and Ideh dadgaran; Responsible for the administrative, technical, and material support as well as the study supervision: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We would like to thank the Vice Chancellor of Research Foundation for financial support. In addition, The authors would like to thank Dr Mohammad Ghaffari for performing statistical analysis and Sana Alavi Nikoo in conducting a literature review and distribution of questionnaire.
References
- Cornu B. New technologies: Integration into education. Berlin: Springer; 1995. [DOI:10.1007/978-0-387-34842-1_2]
- Harden RM, Sowden S, Dunn WR. Educational strategies in curriculum development: The SPICES model. Medical Education. 1984; 18(4):284-97. [DOI:10.1111/j.1365-2923.1984.tb01024.x] [PMID]
- Major CH, Savin Baden M. An introduction to qualitative research synthesis: Managing the information explosion in social science research. London: Routledge; 2010.
- Avramidis E, Norwich B. Teachers’ attitudes towards integration/inclusion: A review of the literature. European Journal of Special Needs Education. 2002; 17(2):129-47. [DOI:10.1080/08856250210129056]
- Harden RM. The integration ladder: A tool for curriculum planning and evaluation. Oxford Medical Education. 2000; 34(7):551-7. [DOI:10.1046/j.1365-2923.2000.00697.x]
- Ward KP. Horizontal integration of the basic sciences in the chiropractic curriculum. Journal of Chiropractic Education. 2010; 24(2):194-7. [DOI:10.7899/1042-5055-24.2.194] [PMID]
- MacLellan WR, Wang Y, Lusis AJ. Systems-based approaches to cardiovascular disease. Nature Reviews Cardiology. 2012; 9(3):172-84. [DOI:10.1038/nrcardio.2011.208] [PMID] [PMCID]
- Dent J, Harden RM, Hunt D. A practical guide for medical teachers. Amesterdam: Elsevier Health Sciences; 2017.
- Yamani N, Shatter Jalali M. Curriculum integration, with emphasis on integration in medical education. Iranian Journal of Medical Education. 2012; 11(9):1202-13.
- Koole S, Vandeweghe S, Mattheos N, De Bruyn H. Implant dentistry education in Europe: 5 years after the association for dental education in Europe consensus report. European Journal of Dental Education. 2014; 18(S1):43-51. [DOI:10.1111/eje.12084] [PMID]
- Rabiee M, Kazennezhad E. Knowledge and attitude of general dentists regarding HIV and Hepatitis infections in Rasht. Research in Medical Education. 2012; 4(1):58-67.
- Manogue M, McLoughlin J, Christersson C, Delap E, Lindh C, Schoonheim Klein M, et al. Curriculum structure, content, learning and assessment in European undergraduate dental education-update 2010. European Journal of Dental Education. 2011; 15(3):133-41. [DOI:10.1111/j.1600-0579.2011.00699.x] [PMID]
- Baghdady MT, Carnahan H, Lam EW, Woods NN. Integration of basic sciences and clinical sciences in oral radiology education for dental students. Journal of Dental Education. 2013; 77(6):757-63. [PMID]
- John MT, Reissmann DR, Čelebić A, Baba K, Kende D, Larsson P, et al. Integration of oral health-related quality of life instruments. Journal of Dentistry. 2016; 53:38-43. [DOI:10.1016/j.jdent.2016.06.006] [PMID] [PMCID]
- Hassanzadeh G, Abolhasani F, Mirzazadeh A, Alizadeh M. [Team-based learning a new strategy in integrated medical curriculum: The experience of school of medicine, Tehran University of Medical Sciences (Persian)]. Iranian Journal of Medical Education. 2013; 13(7):601-10.
Type of Study: Original article |
Subject:
Pathology
Received: 2017/08/23 | Accepted: 2017/12/28 | Published: 2018/03/1
Received: 2017/08/23 | Accepted: 2017/12/28 | Published: 2018/03/1
References
1. Cornu B. New technologies: Integration into education. Berlin: Springer; 1995. [DOI:10.1007/978-0-387-34842-1_2] [DOI:10.1007/978-0-387-34842-1_2]
2. Harden RM, Sowden S, Dunn WR. Educational strategies in curriculum development: The SPICES model. Medical Education. 1984; 18(4):284-97. [DOI:10.1111/j.1365-2923.1984.tb01024.x] [PMID] [DOI:10.1111/j.1365-2923.1984.tb01024.x]
3. Major CH, Savin Baden M. An introduction to qualitative research synthesis: Managing the information explosion in social science research. London: Routledge; 2010.
4. Avramidis E, Norwich B. Teachers' attitudes towards integration/inclusion: A review of the literature. European Journal of Special Needs Education. 2002; 17(2):129-47. [DOI:10.1080/08856250210129056] [DOI:10.1080/08856250210129056]
5. Harden RM. The integration ladder: A tool for curriculum planning and evaluation. Oxford Medical Education. 2000; 34(7):551-7. [DOI:10.1046/j.1365-2923.2000.00697.x] [DOI:10.1046/j.1365-2923.2000.00697.x]
6. Ward KP. Horizontal integration of the basic sciences in the chiropractic curriculum. Journal of Chiropractic Education. 2010; 24(2):194-7. [DOI:10.7899/1042-5055-24.2.194] [PMID] [DOI:10.7899/1042-5055-24.2.194]
7. MacLellan WR, Wang Y, Lusis AJ. Systems-based approaches to cardiovascular disease. Nature Reviews Cardiology. 2012; 9(3):172-84. [DOI:10.1038/nrcardio.2011.208] [PMID] [PMCID] [DOI:10.1038/nrcardio.2011.208]
8. Dent J, Harden RM, Hunt D. A practical guide for medical teachers. Amesterdam: Elsevier Health Sciences; 2017.
9. Yamani N, Shatter Jalali M. Curriculum integration, with emphasis on integration in medical education. Iranian Journal of Medical Education. 2012; 11(9):1202-13.
10. Koole S, Vandeweghe S, Mattheos N, De Bruyn H. Implant dentistry education in Europe: 5 years after the association for dental education in Europe consensus report. European Journal of Dental Education. 2014; 18(S1):43-51. [DOI:10.1111/eje.12084] [PMID] [DOI:10.1111/eje.12084]
11. Rabiee M, Kazennezhad E. Knowledge and attitude of general dentists regarding HIV and Hepatitis infections in Rasht. Research in Medical Education. 2012; 4(1):58-67. [DOI:10.18869/acadpub.rme.4.1.58]
12. Manogue M, McLoughlin J, Christersson C, Delap E, Lindh C, Schoonheim Klein M, et al. Curriculum structure, content, learning and assessment in European undergraduate dental education-update 2010. European Journal of Dental Education. 2011; 15(3):133-41. [DOI:10.1111/j.1600-0579.2011.00699.x] [PMID] [DOI:10.1111/j.1600-0579.2011.00699.x]
13. Baghdady MT, Carnahan H, Lam EW, Woods NN. Integration of basic sciences and clinical sciences in oral radiology education for dental students. Journal of Dental Education. 2013; 77(6):757-63. [PMID] [PMID]
14. John MT, Reissmann DR, Čelebić A, Baba K, Kende D, Larsson P, et al. Integration of oral health-related quality of life instruments. Journal of Dentistry. 2016; 53:38-43. [DOI:10.1016/j.jdent.2016.06.006] [PMID] [PMCID] [DOI:10.1016/j.jdent.2016.06.006]
15. Hassanzadeh G, Abolhasani F, Mirzazadeh A, Alizadeh M. [Team-based learning a new strategy in integrated medical curriculum: The experience of school of medicine, Tehran University of Medical Sciences (Persian)]. Iranian Journal of Medical Education. 2013; 13(7):601-10.
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Zamen Salamati.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
