Fri, Jan 30, 2026
Volume 6, Issue 3 (10-2017)
2017, 6(3): 89-95 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mojarad F, Mahjoub Khatibani S P, Janeshin A. Triple Antibiotic Paste Treatment in Progressive External Root Resorption: A Case Report
. Journal title 2017; 6 (3) :89-95
URL: http://3dj.gums.ac.ir/article-1-285-en.html
URL: http://3dj.gums.ac.ir/article-1-285-en.html


1- Associate Professor, Department of Pediatric Dentistry, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran.
2- Assistant Professor, Dental Science Research Center, Department of Pediatric Dentistry, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran. ,dr.p.mahjoub@gmail.com
3- Assistant Professor, Dental Science Research Center, Department of Pediatric Dentistry, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
2- Assistant Professor, Dental Science Research Center, Department of Pediatric Dentistry, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran. ,
3- Assistant Professor, Dental Science Research Center, Department of Pediatric Dentistry, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 978 kb]
(1427 Downloads)
| Abstract (HTML) (5066 Views)



Full-Text: (3291 Views)
1. Case Report
9-year-old boy was referred to the pediatric department of the Hamadan University of Medical Sciences (Hamadan, Iran) about 1 hour after falling at school, with an avulsed tooth (number 21). The avulsed tooth had been stored in a container carrying tap water. The patient did not show any signs or symptoms of head injury, and his medical history was unremarkable.
Extra-oral examination demonstrated no swelling or pain. Intra-oral examination showed mixed dentition with satisfactory oral hygiene. Left central was avulsed, and a blood clot was found in the alveolar socket. Examination of the tooth socket did not show any fracture of the bony wall or tooth segment. The avulsed tooth had an open apex. Treatment plan and long-term prognosis were discussed with the parents, and a signed written informed consent form was obtained from them for the treatment. The root surface and the socket were rinsed with normal saline. The tooth was carefully placed into the alveolar socket with finger pressure. Then splinting was done with 0.024-inch stainless steel round wire and composite.
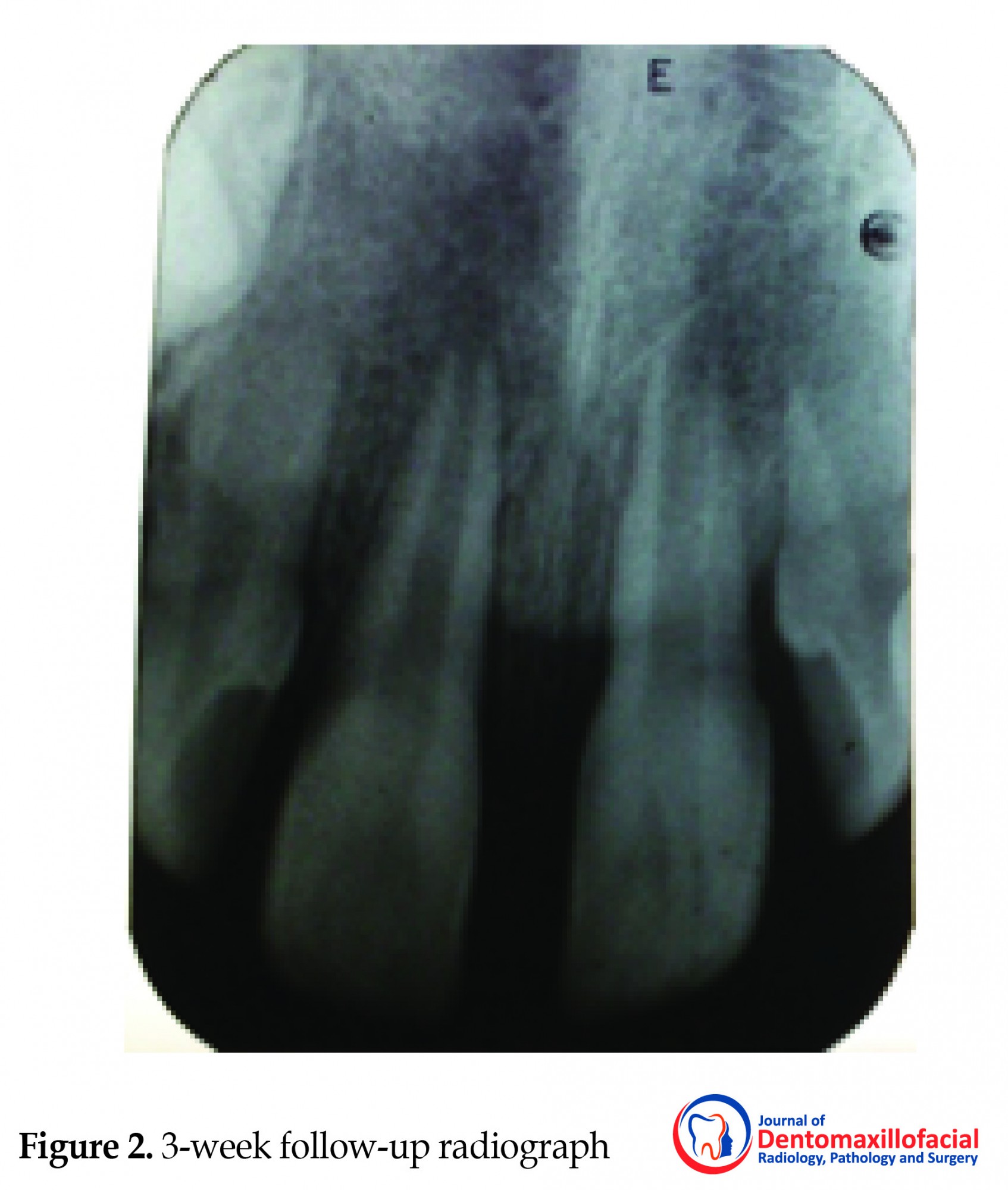
A periapical radiograph was taken to confirm the correctness of the tooth repositioning in the socket (Figure 1). Systemic Amoxicillin 250 mg and 0.2% chlorhexidine mouth rinse were prescribed for one week. The splint was removed after two weeks. The patient was recalled for follow-up examination one week after splint removal. The patient was asymptomatic, and periapical radiograph demonstrated normal periapical tissues (Figure 2). The next patient follow-up examination was planned 6 weeks after the initial visit. At this appointment, the tooth number 21 was found to be tender on percussion. Cold test gave a negative response, suggesting pulp necrosis. An intra-oral periapical radiograph revealed advanced external root resorption in the maxillary left central incisor (Figure 3). Access opening was prepared without local anesthesia, and canal debridement was undertaken. After chemo-mechanical debridement, calcium hydroxide paste was placed in the root canal, and the coronal sealing of access opening was done with reinforced zinc oxide eugenol cement.
9-year-old boy was referred to the pediatric department of the Hamadan University of Medical Sciences (Hamadan, Iran) about 1 hour after falling at school, with an avulsed tooth (number 21). The avulsed tooth had been stored in a container carrying tap water. The patient did not show any signs or symptoms of head injury, and his medical history was unremarkable.
Extra-oral examination demonstrated no swelling or pain. Intra-oral examination showed mixed dentition with satisfactory oral hygiene. Left central was avulsed, and a blood clot was found in the alveolar socket. Examination of the tooth socket did not show any fracture of the bony wall or tooth segment. The avulsed tooth had an open apex. Treatment plan and long-term prognosis were discussed with the parents, and a signed written informed consent form was obtained from them for the treatment. The root surface and the socket were rinsed with normal saline. The tooth was carefully placed into the alveolar socket with finger pressure. Then splinting was done with 0.024-inch stainless steel round wire and composite.
A periapical radiograph was taken to confirm the correctness of the tooth repositioning in the socket (Figure 1). Systemic Amoxicillin 250 mg and 0.2% chlorhexidine mouth rinse were prescribed for one week. The splint was removed after two weeks. The patient was recalled for follow-up examination one week after splint removal. The patient was asymptomatic, and periapical radiograph demonstrated normal periapical tissues (Figure 2). The next patient follow-up examination was planned 6 weeks after the initial visit. At this appointment, the tooth number 21 was found to be tender on percussion. Cold test gave a negative response, suggesting pulp necrosis. An intra-oral periapical radiograph revealed advanced external root resorption in the maxillary left central incisor (Figure 3). Access opening was prepared without local anesthesia, and canal debridement was undertaken. After chemo-mechanical debridement, calcium hydroxide paste was placed in the root canal, and the coronal sealing of access opening was done with reinforced zinc oxide eugenol cement.
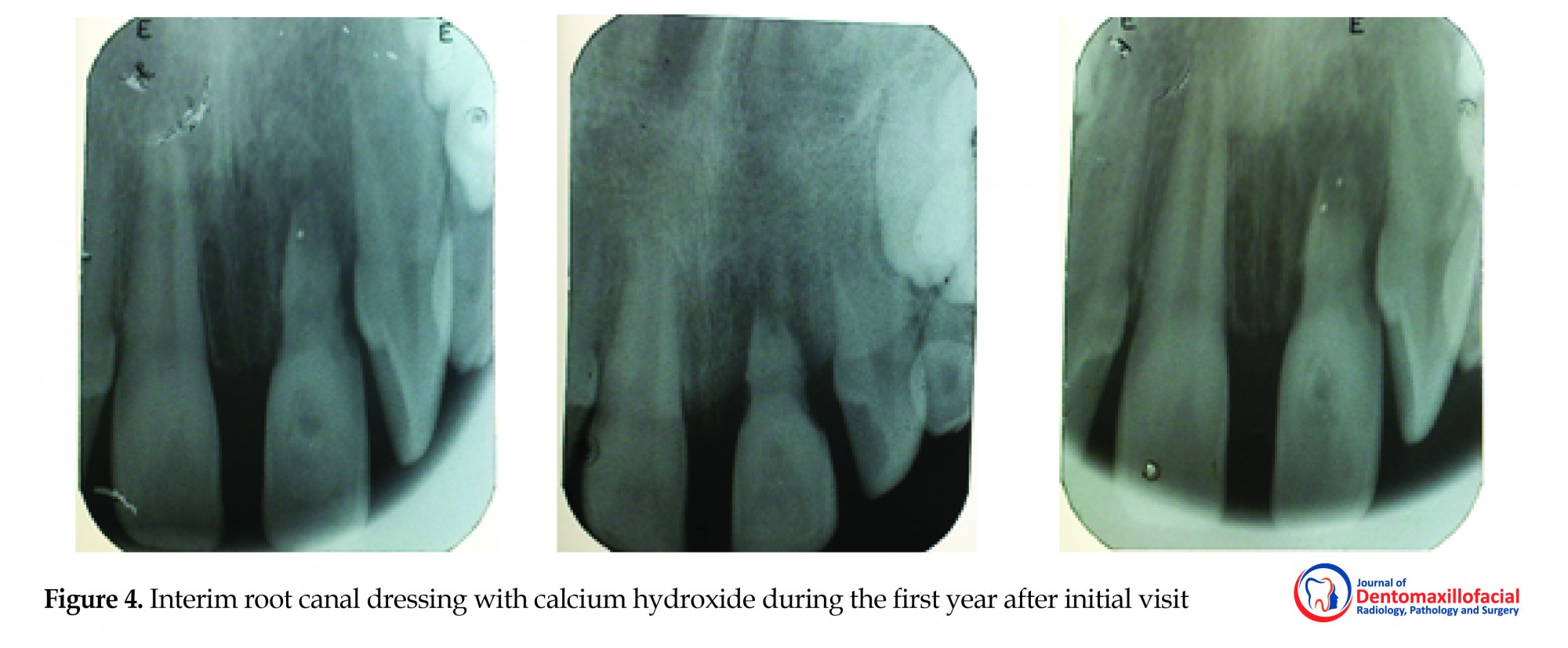
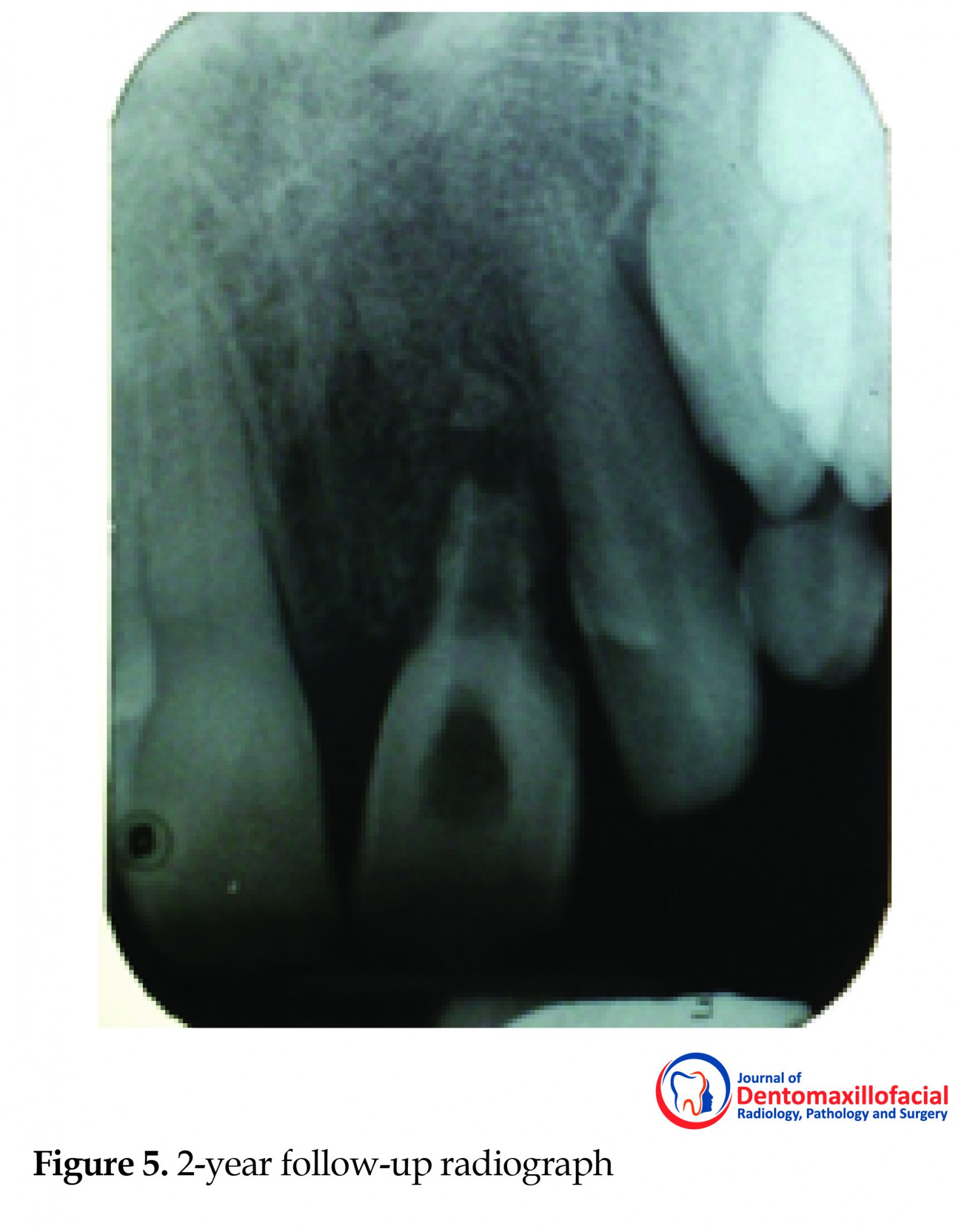
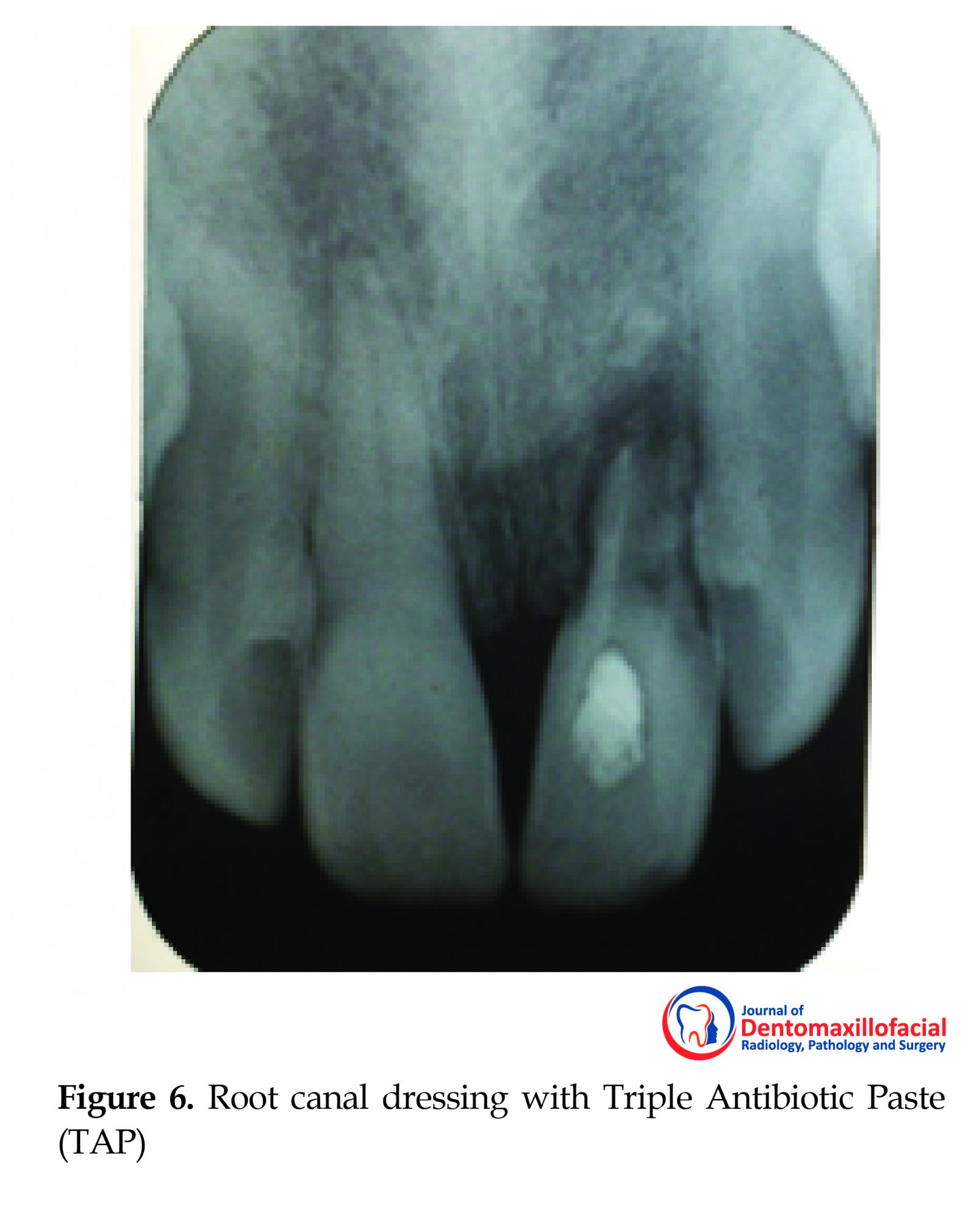
The calcium hydroxide paste was replaced three times during a year because the resorption process was not arrested (Figure 4). Unfortunately, the patient failed to present as scheduled for follow-up appointment during the second year after the initial visit. After two years, the patient came back to the clinic. The tooth coronal seal was compromised. An intra-oral periapical radiograph was taken (Figure 5). According to the consultation with the endodontic department of Hamadan University of Medical Sciences (Hamadan, Iran), the tooth 21 was hopeless due to extensive root resorption and possible root perforation. However, with the parents’ consent, the calcium hydroxide paste was removed and the canal was filled with Triple Antibiotic Paste (TAP) containing metronidazole, ciprofloxacin, and minocycline. The paste was changed monthly for a period of 3 months. After 3 months, the paste was changed for the last time, and it was then allowed to remain in the tooth. The chamber was sealed with resin-modified glass ionomer cement (Figure 6). Follow-up radiograph after 5 years revealed that the external root resorption had been arrested and replacement resorption was observed (Figure 7). In this case, the treatment options before placement of an implant include tooth extraction and space maintenance or preserving the tooth as a space maintainer.
2. Discussion
Tooth avulsion most often occurs in the anterior region of the maxilla, compromising a patient’s esthetic, mechanical and biological functions. The success of its treatment is dependent on several factors including the intensity of the trauma, periodontal ligament vitality, storage media used in the extra-alveolar period, time elapsed between the trauma and replantation, maintenance of pulp vitality, and tooth and alveolus preparation for replantation and endodontic treatment [1, 2]. Ideally, the avulsed tooth should be replanted immediately; if it is not possible, the extra-oral dry time must be minimized by placing the tooth in an appropriate medium before replantation [3].
Suitable media, in order of preference, are Hank’s pH balanced salt solution, Via Span, cold fresh milk, saliva, and physiologic saline [4, 5]. Although tap water is not recommended, it can be used if any of the mentioned storage mediums are not available [6]. In cases of extra-oral dry time of greater than 1 hour, the periodontal ligament is not expected to survive [5]. Pre-treatment of such a tooth with sodium fluoride prior to its replantation will render it more resistant to resorption [7].
In closed apex teeth, prophylactic endodontic therapy should be undertaken within 7-10 days after replantation [8]. However, for teeth with wide open apex, careful observation is recommended as there is a chance for revascularization. If any signs of necrosis such as root resorption are diagnosed, root canal therapy should be performed [9]. In the present case, the avulsed left central had an open apex and was kept in tap water for about 1 hour. It is recommended to soak teeth with open apex in Doxycycline 0.005% for 5 minutes before replantation. It was indicated that revascularization of pulp was significantly enhanced in 40% to 60% of the treated patients [10]. However, due to the unavailability of Doxycycline at the emergency visit, the avulsed tooth was only rinsed with normal saline as usual before replantation.
The tooth was splinted for 2 weeks using acid-etch composite resin and 0.024-inch stainless steel round wire. A semi-rigid splint is the recommended type of splint in avulsion injuries because it allows physiological movement of the tooth during healing and results in decreased incidence of ankylosis [5, 11]. Systemic antibiotics in the form of Amoxicillin 250 mg was prescribed after replantation, but their role in preventing root resorption needs to be elucidated [1]. Pulp necrosis and root resorption are the most common complications resulting from avulsion [6, 9]. The necrotic pulp tissue is susceptible to bacterial contamination. Inflammatory root resorption is directly associated with the periodontium damage at the time of injury and the presence of bacteria within root canal system and dentinal tubules [12]. The denuded root surface resulting from the destruction of the precementum layer and necrosis of cementoblasts allows bacterial toxins inside the root canal system to be transmitted to the periodontium and stimulates an inflammatory response in the periodontal ligament [12-14].
This process can occur rapidly in young patients whose dentinal tubules are wide and allow the irritants to move freely to the external root surface [14]. In the present case, the avulsed tooth was stored in tap water for about an hour, which is a non-physiological storage medium and can preserve periodontal cells viability for 20 minutes [15]. It seems that prolonged tooth storage in tap water led to necrosis of some parts of periodontal ligament, which in turn resulted in denuded root surface being chemotactic to hard tissue resorbing cells. As the avulsed tooth had an open apex at the time of injury and there was a chance of revascularization, endodontic treatment was delayed. However, pulp necrosis occurred.
The combination of prolonged tooth storage in non-physiological medium, presence of infected and necrotic pulp tissue and patient’s young age resulted in rapidly progressive external root resorption 6 weeks after the initial visit. Endodontic therapy to remove the necrotic tissue and long-term calcium hydroxide treatment were planned. Calcium hydroxide is one of the most effective materials for the treatment of external root resorption, and success rates of up to 97% have been reported using this material [4]. There is not a definitive recommendation for the amount of time the calcium hydroxide paste should remain in the canal [16]. Patient cooperation in a long-term calcium hydroxide treatment regimen is a critical factor. With the lack of patient cooperation, a root canal may eventually become infected resulting in possibly tooth loss [17].
In our case, calcium hydroxide was replaced 3 times during the first year after injury because the resorption process was not arrested. The patient failed to present as scheduled for follow-up appointment during the second year after the initial visit. After two years, when the patient came back to the clinic, the tooth coronal seal was compromised. According to the endodontic consultation, the tooth was hopeless at this time. The treatment objective was to retain the avulsed tooth as long as possible to maintain esthetic appearance and occlusal function. In recent years, a new concept has been developed that employs the use of a combination of anti-bacterial drugs (metronidazole, ciprofloxacin, and minocycline) for disinfection of pulpal and periradicular lesions. It has been reported that this mixture can sterilize root dentine [18, 19]. Research with topical antibiotics has shown that this antibiotic combination is effective in killing common endodontic pathogens from necrotic/infected root canals in vitro and in vivo. Moreover, TAP has been used successfully in regenerative endodontic treatments and healing of large periradicular lesions [20-22].
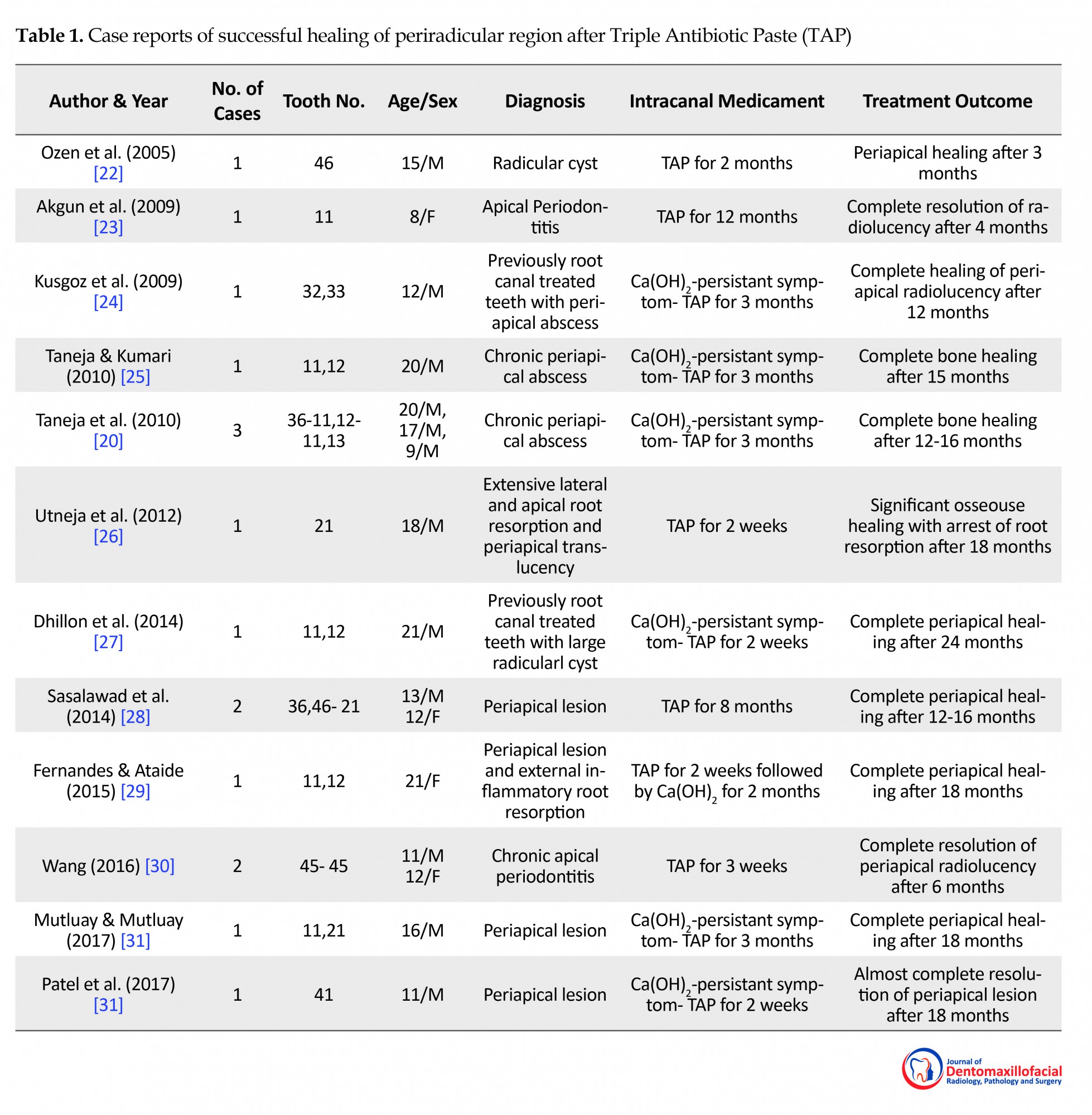
Table 1 shows case reports of successful healing of periradicular region after TAP intracanal medication. In the present case, calcium hydroxide was used, but after two years of clinical and radiographic follow-up, the root resorption was not arrested. The treatment protocol was changed, and TAP was applied to sterilize the root canal system and control inflammatory root resorption. The paste was replaced every month for a period of 3 months. After 3 months, the paste was changed for the last time and it was then allowed to remain in the tooth. The chamber was sealed with resin-modified glass ionomer cement. After its application, the root resorption was arrested. Replacement resorption can occur when inflammatory resorption has been arrested by endodontic treatment. Young patients are more susceptible to replacement resorption due to their high turn-over rate of bone forming cells [8]. After 5 years of clinical and radiographic follow-up, it was observed that inflammatory root resorption had been arrested and replacement resorption took over the resorbed area. Although it is anticipated that the tooth will be lost ultimately by gradual root surface resorption followed by replacement with bone, but it is worth an effort to try maintain the tooth as long as possible for esthetic, functional and psychological rehabilitation of the patients [8]. Several alternative treatments are suggested in the literature including keeping the ankylosed tooth or root, extraction and orthodontic space closure, autotransplantation, implants and other prosthetic treatments. In the present case, the TAP is still in canal and the pulp chamber is sealed with resin-modified glass ionomer. Clinical and radiographical evaluations are still being continued. At 5-year follow-up, the patient was 14 years old and the tooth may be maintained until growth is completed, and other treatment options such as implants or fixed partial dentures can be considered.
Tooth avulsion most often occurs in the anterior region of the maxilla, compromising a patient’s esthetic, mechanical and biological functions. The success of its treatment is dependent on several factors including the intensity of the trauma, periodontal ligament vitality, storage media used in the extra-alveolar period, time elapsed between the trauma and replantation, maintenance of pulp vitality, and tooth and alveolus preparation for replantation and endodontic treatment [1, 2]. Ideally, the avulsed tooth should be replanted immediately; if it is not possible, the extra-oral dry time must be minimized by placing the tooth in an appropriate medium before replantation [3].
Suitable media, in order of preference, are Hank’s pH balanced salt solution, Via Span, cold fresh milk, saliva, and physiologic saline [4, 5]. Although tap water is not recommended, it can be used if any of the mentioned storage mediums are not available [6]. In cases of extra-oral dry time of greater than 1 hour, the periodontal ligament is not expected to survive [5]. Pre-treatment of such a tooth with sodium fluoride prior to its replantation will render it more resistant to resorption [7].
In closed apex teeth, prophylactic endodontic therapy should be undertaken within 7-10 days after replantation [8]. However, for teeth with wide open apex, careful observation is recommended as there is a chance for revascularization. If any signs of necrosis such as root resorption are diagnosed, root canal therapy should be performed [9]. In the present case, the avulsed left central had an open apex and was kept in tap water for about 1 hour. It is recommended to soak teeth with open apex in Doxycycline 0.005% for 5 minutes before replantation. It was indicated that revascularization of pulp was significantly enhanced in 40% to 60% of the treated patients [10]. However, due to the unavailability of Doxycycline at the emergency visit, the avulsed tooth was only rinsed with normal saline as usual before replantation.
The tooth was splinted for 2 weeks using acid-etch composite resin and 0.024-inch stainless steel round wire. A semi-rigid splint is the recommended type of splint in avulsion injuries because it allows physiological movement of the tooth during healing and results in decreased incidence of ankylosis [5, 11]. Systemic antibiotics in the form of Amoxicillin 250 mg was prescribed after replantation, but their role in preventing root resorption needs to be elucidated [1]. Pulp necrosis and root resorption are the most common complications resulting from avulsion [6, 9]. The necrotic pulp tissue is susceptible to bacterial contamination. Inflammatory root resorption is directly associated with the periodontium damage at the time of injury and the presence of bacteria within root canal system and dentinal tubules [12]. The denuded root surface resulting from the destruction of the precementum layer and necrosis of cementoblasts allows bacterial toxins inside the root canal system to be transmitted to the periodontium and stimulates an inflammatory response in the periodontal ligament [12-14].
This process can occur rapidly in young patients whose dentinal tubules are wide and allow the irritants to move freely to the external root surface [14]. In the present case, the avulsed tooth was stored in tap water for about an hour, which is a non-physiological storage medium and can preserve periodontal cells viability for 20 minutes [15]. It seems that prolonged tooth storage in tap water led to necrosis of some parts of periodontal ligament, which in turn resulted in denuded root surface being chemotactic to hard tissue resorbing cells. As the avulsed tooth had an open apex at the time of injury and there was a chance of revascularization, endodontic treatment was delayed. However, pulp necrosis occurred.
The combination of prolonged tooth storage in non-physiological medium, presence of infected and necrotic pulp tissue and patient’s young age resulted in rapidly progressive external root resorption 6 weeks after the initial visit. Endodontic therapy to remove the necrotic tissue and long-term calcium hydroxide treatment were planned. Calcium hydroxide is one of the most effective materials for the treatment of external root resorption, and success rates of up to 97% have been reported using this material [4]. There is not a definitive recommendation for the amount of time the calcium hydroxide paste should remain in the canal [16]. Patient cooperation in a long-term calcium hydroxide treatment regimen is a critical factor. With the lack of patient cooperation, a root canal may eventually become infected resulting in possibly tooth loss [17].
In our case, calcium hydroxide was replaced 3 times during the first year after injury because the resorption process was not arrested. The patient failed to present as scheduled for follow-up appointment during the second year after the initial visit. After two years, when the patient came back to the clinic, the tooth coronal seal was compromised. According to the endodontic consultation, the tooth was hopeless at this time. The treatment objective was to retain the avulsed tooth as long as possible to maintain esthetic appearance and occlusal function. In recent years, a new concept has been developed that employs the use of a combination of anti-bacterial drugs (metronidazole, ciprofloxacin, and minocycline) for disinfection of pulpal and periradicular lesions. It has been reported that this mixture can sterilize root dentine [18, 19]. Research with topical antibiotics has shown that this antibiotic combination is effective in killing common endodontic pathogens from necrotic/infected root canals in vitro and in vivo. Moreover, TAP has been used successfully in regenerative endodontic treatments and healing of large periradicular lesions [20-22].
Table 1 shows case reports of successful healing of periradicular region after TAP intracanal medication. In the present case, calcium hydroxide was used, but after two years of clinical and radiographic follow-up, the root resorption was not arrested. The treatment protocol was changed, and TAP was applied to sterilize the root canal system and control inflammatory root resorption. The paste was replaced every month for a period of 3 months. After 3 months, the paste was changed for the last time and it was then allowed to remain in the tooth. The chamber was sealed with resin-modified glass ionomer cement. After its application, the root resorption was arrested. Replacement resorption can occur when inflammatory resorption has been arrested by endodontic treatment. Young patients are more susceptible to replacement resorption due to their high turn-over rate of bone forming cells [8]. After 5 years of clinical and radiographic follow-up, it was observed that inflammatory root resorption had been arrested and replacement resorption took over the resorbed area. Although it is anticipated that the tooth will be lost ultimately by gradual root surface resorption followed by replacement with bone, but it is worth an effort to try maintain the tooth as long as possible for esthetic, functional and psychological rehabilitation of the patients [8]. Several alternative treatments are suggested in the literature including keeping the ankylosed tooth or root, extraction and orthodontic space closure, autotransplantation, implants and other prosthetic treatments. In the present case, the TAP is still in canal and the pulp chamber is sealed with resin-modified glass ionomer. Clinical and radiographical evaluations are still being continued. At 5-year follow-up, the patient was 14 years old and the tooth may be maintained until growth is completed, and other treatment options such as implants or fixed partial dentures can be considered.
3. Conclusion
Root resorption is common in avulsed replanted teeth. In the present case, as calcium hydroxide failed to arrest the resorption process, TAP was used as an alternative that was successful. Although replacement resorption took over the resorbed area, the tooth is still in a stable and functional situation after 5 years of follow-up.
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declared no conflicts of interest
References
Root resorption is common in avulsed replanted teeth. In the present case, as calcium hydroxide failed to arrest the resorption process, TAP was used as an alternative that was successful. Although replacement resorption took over the resorbed area, the tooth is still in a stable and functional situation after 5 years of follow-up.
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declared no conflicts of interest
References
- Dhillon JS, Narula NB, Kumar M. Complete root resorption after reimplantation of maxillary central incisor- A case report. Endodontology. 2011; 23(2):98-103.
- Andreasen JO. Relationship between cell damage in the periodontal ligament after replantation and subsequent development of root resorption. A time-related study in monkeys. Acta Odontologica Scandinavica. 1981; 39(1):15–25. doi: 10.3109/00016358109162254
- Andreasen JO, Borum MK, Andreasen FM. Replantation of 400 avulsed permanent incisors. Factors related to root growth. EDental Traumatology. 1995; 11(2):69-75. doi: 10.1111/j.1600-9657.1995.tb00463.x
- Finucane D, Kinirons MJ. External inflammatory and replacement resorption of luxated and avulsed replanted permanent incisors: A review and case presentation. Dental Traumatology. 2003; 19(3):170-4. doi: 10.1034/j.1600-9657.2003.00154.x
- Trope M. Luxation injuries and external root resorption- Etiology, treatment and prognosis. Journal of the California Dental Association. 2000; 28(11):860-6. PMID: 11811235
- Ram D, Cohenca N. Therapeutic protocols for avulsed permanent teeth: review and clinical update. Pediatric Dentistry. 2004; 26(3):251-5. PMID: 15185807
- Sardana D, Goyal A, Gauba K. Delayed replantation of avulsed tooth with 15-hours extra-0ral time: 3-year follow-up. Singapore Dental Journal. 2014; 35:71-6. doi: 10.1016/j.sdj.2014.04.001
- Hegde MN, Pardal D. Healing of external inflammatory root resorption – a case report. Endodontology. 2007; 19(1):34-8.
- Moradin H, Badakhsh S, Rahimi M, Hekmatfar S. Replantation of an avulsed maxillary incisor after 12 hours: Three-year follow-up. Iranian Endodontic Journal. 2013; 8(1):33-6. doi: 10.22037/iej.v8i1.2728
- Cvek M, Cleaton-Jones P, Austin J, Lownie J, King M, Fatti P. Effect of topical application of doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisors. Dental Traumatology. 1990; 6(4):170–6. doi: 10.1111/j.1600-9657.1990.tb00413.
- Andreasen JO, Andreasen FM. Avulsion. In: Andreasen JO AF, editor. Textbook and color atlas of traumatic injuries to the teeth. Copenhagen: Blackwell Munksgaard; 2007.
- Trope M, Yesiloy C, Koren L, Moshonov J, Friedman S. Effect of different endodontic treatment protocols on periodontal repair and root resorption of replanted dog teeth. Journal of Endodontics. 1992; 18(10):492–6. doi: 10.1016/s0099-2399(06)81349-x
- Fuss Z, Tsesis I, Lin S. Root resorption—Diagnosis, classification and treatment choices based on stimulation factors. Dental Traumatology. 2003; 19(4):175-82. doi: 10.1034/j.1600-9657.2003.00192.x
- Trope M. Clinical management of the avulsed tooth: present strategies and future directions. Dental Traumatology. 2002; 18(1):1–11. doi: 10.1046/j.1600-4469.2001.00001.x
- Gomes MCB, Westphalen VPD, Westphalen FH, Silva Neto UX, Fariniuk LF, Carneiro E. Study of storage media for avulsed teeth. Study of Storage Media for Avulsed Teeth. 2009;1(2):69-76.
- Karp J, Bryk J, Menke E, McTigue D. The complete endodontic obturation of an avulsed immature permanent incisor with mineral trioxide aggregate: A case report. Pediatric Dentistry. 2006; 28(3):273-8. PMID: 16805362
- Martins WD, Westphalen VP, Westphalen FH. Tooth replantation after traumatic avulsion: A 27-year follow-up. Dental Traumatology. 2004; 20(2):101–5. doi: 10.1111/j.1600-4469.2004.00224.x
- Murvindran V, Raj JD. Antibiotics as an Intracanal Medicament in Endodontics. Journal of Pharmaceutical Sciences and Research. 2014; 6(9):297-301.
- Abbott PV. Medicaments: Aids to success in endodontics. Part 1. A review of the literature. Australian Dental Journal. 1990; 35(5):438-48. doi: 10.1111/j.1834-7819.1990.tb05427.x
- Taneja S, Kumari M, Parkash H. Nonsurgical healing of large periradicular lesions using a triple antibiotic paste: A case series. Contemporary Clinical Dentistry. 2010; 1(1):31-5. doi: 10.4103/0976-237x.62519
- Er K, Kustarci A, Ozan U, Tasdemir T. Nonsurgical endodontic treatment of dens invaginatus in a mandibular premolar with a large periradicular lesion. A case report. Journal of Endodontics. 2007; 33(3):322–4. doi: 10.1016/j.joen.2006.09.001
- Ozan U, Er K. Endodontic treatment of a large cyst like periradicular lesion using a combination of antibiotic drugs: A case report. Journal of Endodontics. 2005; 31(12):898–900. doi: 10.1097/01.don.0000164129.74235.8e
- Akgun OM, Altun C, Guven G. Use of triple antibiotic paste as a disinfectant for a traumatized immature tooth with a periapical lesion: A case report. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2009; 108(2):e62–e65. doi: 10.1016/j.tripleo.2009.04.015
- Kusgoz A, Yildirim T, Er K,Arslan I. Retreatment of a resected tooth associated with a large periradicular lesion by using a triple antibiotic paste and mineral trioxide aggregate: a case report with a thirty-month follow-up. Journal of Endodontics. 2009; 35(11):1603-6. doi: 10.1016/j.joen.2009.07.019
- Taneja S, Kumari M. Use of triple antibiotic paste in the treatment of large periradicular lesions. Journal of Investigative and Clinical Dentistry. 2012; 3(1):72-6. doi: 10.1111/j.2041-1626.2011.00082.x
- Utneja S, Garg G, Arora S, Talwar S. Nonsurgical endodontic retreatment of advanced inflammatory external root resorption usingmineral trioxide aggregate obturation. Case Reports in Dentistry. 2012; 2012:624792. doi: 10.1155/2012/624792
- Dhillon J, Gill B, Ratol S, Saini S, Amita, Bedi H. Healing of a large periapical lesion using triple antibiotic paste and intracanal aspiration in nonsurgical endodontic retreatment. Indian Journal of Dentistry. 2014; 5(3):161-5. doi: 10.4103/0975-962x.140843
- Sasalawad SS, Naik SN, Poornima P, Shashibhushan KK. Nonsurgical healing of large periradicular lesions using a triple antibiotic paste. Indian Journal of Oral Sciences. 2014; 5(3):146-50. doi: 10.4103/0976-6944.144539
- Fernandes M, Ataide ID. Nonsurgical management of a large periapical lesion associated with an immature tooth displaying external inflammatory resorption. Journal of Conservative Dentistry. 2015; 18(4):349-53. doi: 10.4103/0972-0707.159758
- Wang HJ, Melody Chen YH, Chen KL. Conservative treatment of immature teeth with apical periodontitis using triple antibiotic paste disinfection. Journal of Dental Sciences. 2016; 11(2):196–201. doi: 10.1016/j.jds.2013.02.029
- Mutluay AT and Mutluay M. Management of large periapical lesion due to trauma using triple antibiotic paste. Journal of Oral and Maxillofacial Radiology. 2017; 5(2):58-61. doi: 10.4103/jomr.jomr_19_17
Type of Study: Original article |
Subject:
So on
Received: 2017/05/16 | Accepted: 2017/07/20 | Published: 2017/10/1
Received: 2017/05/16 | Accepted: 2017/07/20 | Published: 2017/10/1
References
1. Dhillon JS, Narula NB, Kumar M. Complete root resorption after reimplantation of maxillary central incisor- A case report. Endodontology. 2011; 23(2):98-103.
2. Andreasen JO. Relationship between cell damage in the periodontal ligament after replantation and subsequent development of root resorption. A time-related study in monkeys. Acta Odontologica Scandinavica. 1981; 39(1):15–25. doi: 10.3109/00016358109162254 [DOI:10.3109/00016358109162254]
3. Andreasen JO, Borum MK, Andreasen FM. Replantation of 400 avulsed permanent incisors. Factors related to root growth. EDental Traumatology. 1995; 11(2):69-75. doi: 10.1111/j.1600-9657.1995.tb00463.x [DOI:10.1111/j.1600-9657.1995.tb00463.x]
4. Finucane D, Kinirons MJ. External inflammatory and replacement resorption of luxated and avulsed replanted permanent incisors: A review and case presentation. Dental Traumatology. 2003; 19(3):170-4. doi: 10.1034/j.1600-9657.2003.00154.x [DOI:10.1034/j.1600-9657.2003.00154.x]
5. Trope M. Luxation injuries and external root resorption- Etiology, treatment and prognosis. Journal of the California Dental Association. 2000; 28(11):860-6. PMID: 11811235 [PMID]
6. Ram D, Cohenca N. Therapeutic protocols for avulsed permanent teeth: review and clinical update. Pediatric Dentistry. 2004; 26(3):251-5. PMID: 15185807 [PMID]
7. Sardana D, Goyal A, Gauba K. Delayed replantation of avulsed tooth with 15-hours extra-0ral time: 3-year follow-up. Singapore Dental Journal. 2014; 35:71-6. doi: 10.1016/j.sdj.2014.04.001 [DOI:10.1016/j.sdj.2014.04.001]
8. Hegde MN, Pardal D. Healing of external inflammatory root resorption – a case report. Endodontology. 2007; 19(1):34-8.
9. Moradin H, Badakhsh S, Rahimi M, Hekmatfar S. Replantation of an avulsed maxillary incisor after 12 hours: Three-year follow-up. Iranian Endodontic Journal. 2013; 8(1):33-6. doi: 10.22037/iej.v8i1.2728
10. Cvek M, Cleaton-Jones P, Austin J, Lownie J, King M, Fatti P. Effect of topical application of doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisors. Dental Traumatology. 1990; 6(4):170–6. doi: 10.1111/j.1600-9657.1990.tb00413.
11. Andreasen JO, Andreasen FM. Avulsion. In: Andreasen JO AF, editor. Textbook and color atlas of traumatic injuries to the teeth. Copenhagen: Blackwell Munksgaard; 2007.
12. Trope M, Yesiloy C, Koren L, Moshonov J, Friedman S. Effect of different endodontic treatment protocols on periodontal repair and root resorption of replanted dog teeth. Journal of Endodontics. 1992; 18(10):492–6. doi: 10.1016/s0099-2399(06)81349-x [DOI:10.1016/S0099-2399(06)81349-X]
13. Fuss Z, Tsesis I, Lin S. Root resorption—Diagnosis, classification and treatment choices based on stimulation factors. Dental Traumatology. 2003; 19(4):175-82. doi: 10.1034/j.1600-9657.2003.00192.x [DOI:10.1034/j.1600-9657.2003.00192.x]
14. Trope M. Clinical management of the avulsed tooth: present strategies and future directions. Dental Traumatology. 2002; 18(1):1–11. doi: 10.1046/j.1600-4469.2001.00001.x [DOI:10.1046/j.1600-4469.2001.00001.x]
15. Gomes MCB, Westphalen VPD, Westphalen FH, Silva Neto UX, Fariniuk LF, Carneiro E. Study of storage media for avulsed teeth. Study of Storage Media for Avulsed Teeth. 2009;1(2):69-76.
16. Karp J, Bryk J, Menke E, McTigue D. The complete endodontic obturation of an avulsed immature permanent incisor with mineral trioxide aggregate: A case report. Pediatric Dentistry. 2006; 28(3):273-8. PMID: 16805362 [PMID]
17. Martins WD, Westphalen VP, Westphalen FH. Tooth replantation after traumatic avulsion: A 27-year follow-up. Dental Traumatology. 2004; 20(2):101–5. doi: 10.1111/j.1600-4469.2004.00224.x [DOI:10.1111/j.1600-4469.2004.00224.x]
18. Murvindran V, Raj JD. Antibiotics as an Intracanal Medicament in Endodontics. Journal of Pharmaceutical Sciences and Research. 2014; 6(9):297-301.
19. Abbott PV. Medicaments: Aids to success in endodontics. Part 1. A review of the literature. Australian Dental Journal. 1990; 35(5):438-48. doi: 10.1111/j.1834-7819.1990.tb05427.x [DOI:10.1111/j.1834-7819.1990.tb05427.x]
20. Taneja S, Kumari M, Parkash H. Nonsurgical healing of large periradicular lesions using a triple antibiotic paste: A case series. Contemporary Clinical Dentistry. 2010; 1(1):31-5. doi: 10.4103/0976-237x.62519 [DOI:10.4103/0976-237X.62519]
21. Er K, Kustarci A, Ozan U, Tasdemir T. Nonsurgical endodontic treatment of dens invaginatus in a mandibular premolar with a large periradicular lesion. A case report. Journal of Endodontics. 2007; 33(3):322–4. doi: 10.1016/j.joen.2006.09.001 [DOI:10.1016/j.joen.2006.09.001]
22. Ozan U, Er K. Endodontic treatment of a large cyst like periradicular lesion using a combination of antibiotic drugs: A case report. Journal of Endodontics. 2005; 31(12):898–900. doi: 10.1097/01.don.0000164129.74235.8e [DOI:10.1097/01.don.0000164129.74235.8e]
23. Akgun OM, Altun C, Guven G. Use of triple antibiotic paste as a disinfectant for a traumatized immature tooth with a periapical lesion: A case report. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2009; 108(2):e62–e65. doi: 10.1016/j.tripleo.2009.04.015 [DOI:10.1016/j.tripleo.2009.04.015]
24. Kusgoz A, Yildirim T, Er K,Arslan I. Retreatment of a resected tooth associated with a large periradicular lesion by using a triple antibiotic paste and mineral trioxide aggregate: a case report with a thirty-month follow-up. Journal of Endodontics. 2009; 35(11):1603-6. doi: 10.1016/j.joen.2009.07.019 [DOI:10.1016/j.joen.2009.07.019]
25. Taneja S, Kumari M. Use of triple antibiotic paste in the treatment of large periradicular lesions. Journal of Investigative and Clinical Dentistry. 2012; 3(1):72-6. doi: 10.1111/j.2041-1626.2011.00082.x [DOI:10.1111/j.2041-1626.2011.00082.x]
26. Utneja S, Garg G, Arora S, Talwar S. Nonsurgical endodontic retreatment of advanced inflammatory external root resorption usingmineral trioxide aggregate obturation. Case Reports in Dentistry. 2012; 2012:624792. doi: 10.1155/2012/624792 [DOI:10.1155/2012/624792]
27. Dhillon J, Gill B, Ratol S, Saini S, Amita, Bedi H. Healing of a large periapical lesion using triple antibiotic paste and intracanal aspiration in nonsurgical endodontic retreatment. Indian Journal of Dentistry. 2014; 5(3):161-5. doi: 10.4103/0975-962x.140843 [DOI:10.4103/0975-962X.140843]
28. Sasalawad SS, Naik SN, Poornima P, Shashibhushan KK. Nonsurgical healing of large periradicular lesions using a triple antibiotic paste. Indian Journal of Oral Sciences. 2014; 5(3):146-50. doi: 10.4103/0976-6944.144539 [DOI:10.4103/0976-6944.144539]
29. Fernandes M, Ataide ID. Nonsurgical management of a large periapical lesion associated with an immature tooth displaying external inflammatory resorption. Journal of Conservative Dentistry. 2015; 18(4):349-53. doi: 10.4103/0972-0707.159758 [DOI:10.4103/0972-0707.159758]
30. Wang HJ, Melody Chen YH, Chen KL. Conservative treatment of immature teeth with apical periodontitis using triple antibiotic paste disinfection. Journal of Dental Sciences. 2016; 11(2):196–201. doi: 10.1016/j.jds.2013.02.029 [DOI:10.1016/j.jds.2013.02.029]
31. Mutluay AT and Mutluay M. Management of large periapical lesion due to trauma using triple antibiotic paste. Journal of Oral and Maxillofacial Radiology. 2017; 5(2):58-61. doi: 10.4103/jomr.jomr_19_17
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Zamen Salamati.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
