Fri, Apr 26, 2024
Volume 6, Issue 3 (10-2017)
2017, 6(3): 43-48 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gholinia F, Khalighi Sigarudi A, Ghavami Lahij Y. Indications for Prophylactic Removal of Unerupted Asymptomatic Pathology-free Third Molars Referred by Iranian Orthodontists. Journal title 2017; 6 (3) :43-48
URL: http://3dj.gums.ac.ir/article-1-279-en.html
URL: http://3dj.gums.ac.ir/article-1-279-en.html


1- Professor, Department of Orthodontics, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
2- Professor, Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
3- DDS, Department of Dentistry, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran. , yghl90@yahoo.com
2- Professor, Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
3- DDS, Department of Dentistry, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran. , yghl90@yahoo.com
Full-Text [PDF 673 kb]
(883 Downloads)
| Abstract (HTML) (3905 Views)
4. Discussion
The current study aimed to evaluate the opinion of Iranian orthodontists, and the relationship between their decision-making process and some variables as their different cultures, place of graduation, sex and professional practice experience.
In 2009, Eser Tüfekçia et al. [13, 16] compared Swedish orthodontists’ opinions about the role of erupting third molars as a cause of dental crowding with their fellow American orthodontists. They found that most of the American and Swedish orthodontists believe that third molar eruption exerts an anterior force. In spite of this belief, they think that these teeth “rarely” or “never” cause late crowding. In 2007, Steven et al. [14, 10] reported that orthodontists and oral surgeons point of view, mandibular third molars are more likely to cause late crowding and because of that they often remove these teeth prophylactically.
We found that although 21.2% of orthodontists in Iran believe that third molar can cause late crowding but only 3.8% of them referred their patients for prophylactic removal to prevent future relapses. They believe that late crowding concern results in mandibular third molar removal in comparison to maxillary third molar. This finding is consistent with the results of three other studies conducted by Steven et al., Eser Tüfekçia et al., and Snug Jin Kin et al. [13, 14, 16, 10].
This study also showed that the clinicians’ sex and their place of graduation could affect their decision-making. It was indicated that almost every man agreed with the idea of third molar removal if it did not have any antagonist tooth, and most of the men disagreed with prophylactic removal because of patient’s request. About the place of graduation, most clinicians who had studied in Iran, were in agreement with asymptomatic pathologic-free third molar removal and the striking reason was lack of space.
5. Conclusion
According to the answers of Iranian orthodontists, the three most significant reasons for asymptomatic pathology-free third molar removal are deviation in eruption path, lack of space in posterior region, and lack of antagonist. Mandibular third molar is usually extracted to prevent late anterior crowding. Although 21.2% of orthodontists believe that third molar can cause late anterior crowding, only 3.8% of them referred these cases. Variables such as sex and place of graduation affected clinicians’ decision. Out of the study participants, all the male one and all aged between 30 and 39 years were in agreement with third molar removal due to lack of space.
Acknowledgments
This study was designed as a thesis for Doctoral Degree in General Dentistry and all the expenses were paid by the authors themselves.
Conflict of Interest
The authors declared no conflicts of interest.
References
Full-Text: (908 Views)
1. Introduction
Third molars usually first appear on radiograph of people aged 5 to 16 year [1, 2]. They often have a mesial inclination at first which then progressively becomes upright and generally erupts between 18 and 24 years of age [3-5]. Being the last teeth to erupt, they are usually impacted due to lack of space [6]. Impacted wisdom teeth may be either symptomatic or asymptomatic. Both conditions may associate with pathological changes such as pericoronitis, periodontitis, root resorption, caries, cysts, or tumors. If third molar is associated with pathological changes or pain; then the choice of treatment is surgical removal [7].
Prophylactic removal of impacted asymptomatic disease-free third molars is defined as a surgical procedure in which the patient dose not present or has not presented any symptoms or pathologies associated with these third molars [8, 9]. Regardless of numerous attempts to describe the role of third molars in causing late anterior crowding, the issue is still controversial [8, 10]. Despite general consensus on symptomatic impacted third molar removal, the management of asymptomatic impacted wisdom teeth remains a controversial issue. Orthodontists are often involved in making a proper decision for such teeth management. Majority of orthodontic patients have asymptomatic impacted wisdom teeth, which some of them eventually should be extracted for orthodontic reasons or to complete orthodontic therapy [9, 10]. Each decisions on this issue, e.g., retention versus prophylactic removal of these teeth, should be based on scientific evidence [11, 12].
Guidelines for the removal of both symptomatic and pathologic third molars and asymptomatic pathology-free third molars are justified. However, routine asymptomatic third molar removal fails the test of evidence-based dentistry and is in contrast with our primary obligation as doctors to “do no harm.” Although in the mid-20th century some authors recommended early extraction of all third molars, in the 21st century the routine removal of asymptomatic pathology-free third molars is outdated and an invalid excuse [12-15].This study aimed to review the indications for referral of unerupted asymptomatic pathology-free third molar prophylactic removal by Iranian orthodontists. This study could help us evaluate the efficacy of supplemental courses in this field in Iran.
2. Materials and Methods
A survey consisting of three parts was developed, which required some personal information of the participants such as sex, age, etc. In the first part, there are questions related to the indications of referral for third molar removal. The second and the last part contained 12 panoramic radiographs containing impacted third molars in either upper or lower jaw to evaluate the orthodontists’ judgments. To verify the content validity (CVI and CVR) of the survey, we called the professional evaluation of a panel of orthodontists in Guilan University of Medical Sciences. According to the evaluation, the CVR was low (<0.62) only for the fourth radiograph, which was replaced with another one and CVI of one of the questions had borderline score (74%), which was revised. All other items had strong validity index (CVI>90%).
The survey was designed using Google account as an internet survey tool and distributed to all orthodontists in Iran in 2017. E-mail addresses of the orthodontists were obtained from web pages of the dental schools in Iran and Iranian association of orthodontists (n=304). Follow up E-mail were sent three times within a period of 2 months, too. Kruskal-Wallis and Mann-Whitney analyses were used to determine the differences in responses to questions with respect to the clinicians’ professional practice experience, age, sex, and the place of graduation. P value less than 0.05 was considered significant.
3. Results
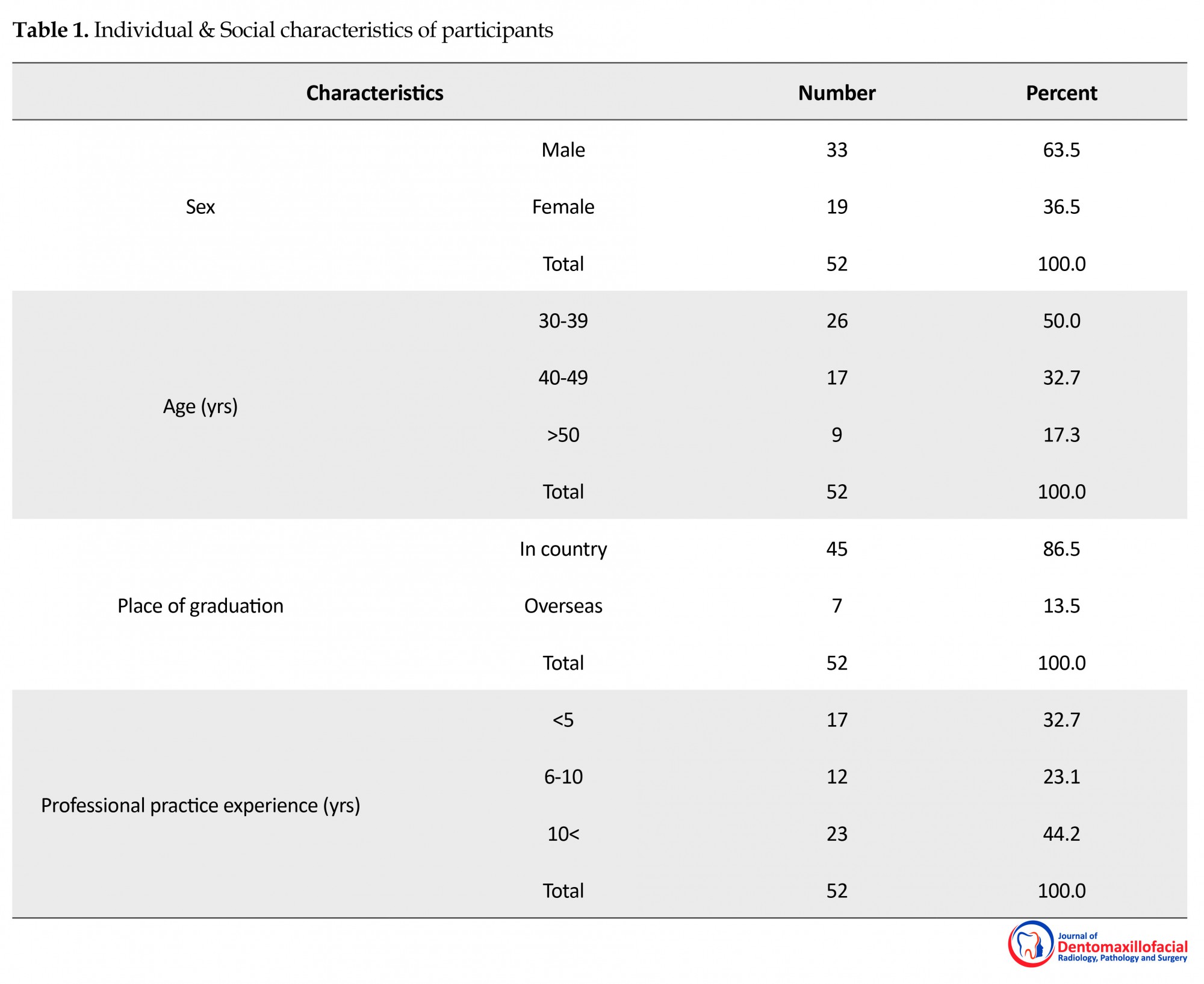
Of 304 questionnaires that were sent, only 52 returned with answer. Men constituted 63.5% of the sample and 36.5% were women. The mean (SD) age of respondents was 40.9(8.9) years and their mean (SD) professional practice experience was 10.8(7.8) years. Of the total participants, 86.5% studied in Iran and 13.5% in overseas (Table 1).
Third molars usually first appear on radiograph of people aged 5 to 16 year [1, 2]. They often have a mesial inclination at first which then progressively becomes upright and generally erupts between 18 and 24 years of age [3-5]. Being the last teeth to erupt, they are usually impacted due to lack of space [6]. Impacted wisdom teeth may be either symptomatic or asymptomatic. Both conditions may associate with pathological changes such as pericoronitis, periodontitis, root resorption, caries, cysts, or tumors. If third molar is associated with pathological changes or pain; then the choice of treatment is surgical removal [7].
Prophylactic removal of impacted asymptomatic disease-free third molars is defined as a surgical procedure in which the patient dose not present or has not presented any symptoms or pathologies associated with these third molars [8, 9]. Regardless of numerous attempts to describe the role of third molars in causing late anterior crowding, the issue is still controversial [8, 10]. Despite general consensus on symptomatic impacted third molar removal, the management of asymptomatic impacted wisdom teeth remains a controversial issue. Orthodontists are often involved in making a proper decision for such teeth management. Majority of orthodontic patients have asymptomatic impacted wisdom teeth, which some of them eventually should be extracted for orthodontic reasons or to complete orthodontic therapy [9, 10]. Each decisions on this issue, e.g., retention versus prophylactic removal of these teeth, should be based on scientific evidence [11, 12].
Guidelines for the removal of both symptomatic and pathologic third molars and asymptomatic pathology-free third molars are justified. However, routine asymptomatic third molar removal fails the test of evidence-based dentistry and is in contrast with our primary obligation as doctors to “do no harm.” Although in the mid-20th century some authors recommended early extraction of all third molars, in the 21st century the routine removal of asymptomatic pathology-free third molars is outdated and an invalid excuse [12-15].This study aimed to review the indications for referral of unerupted asymptomatic pathology-free third molar prophylactic removal by Iranian orthodontists. This study could help us evaluate the efficacy of supplemental courses in this field in Iran.
2. Materials and Methods
A survey consisting of three parts was developed, which required some personal information of the participants such as sex, age, etc. In the first part, there are questions related to the indications of referral for third molar removal. The second and the last part contained 12 panoramic radiographs containing impacted third molars in either upper or lower jaw to evaluate the orthodontists’ judgments. To verify the content validity (CVI and CVR) of the survey, we called the professional evaluation of a panel of orthodontists in Guilan University of Medical Sciences. According to the evaluation, the CVR was low (<0.62) only for the fourth radiograph, which was replaced with another one and CVI of one of the questions had borderline score (74%), which was revised. All other items had strong validity index (CVI>90%).
The survey was designed using Google account as an internet survey tool and distributed to all orthodontists in Iran in 2017. E-mail addresses of the orthodontists were obtained from web pages of the dental schools in Iran and Iranian association of orthodontists (n=304). Follow up E-mail were sent three times within a period of 2 months, too. Kruskal-Wallis and Mann-Whitney analyses were used to determine the differences in responses to questions with respect to the clinicians’ professional practice experience, age, sex, and the place of graduation. P value less than 0.05 was considered significant.
3. Results
Of 304 questionnaires that were sent, only 52 returned with answer. Men constituted 63.5% of the sample and 36.5% were women. The mean (SD) age of respondents was 40.9(8.9) years and their mean (SD) professional practice experience was 10.8(7.8) years. Of the total participants, 86.5% studied in Iran and 13.5% in overseas (Table 1).
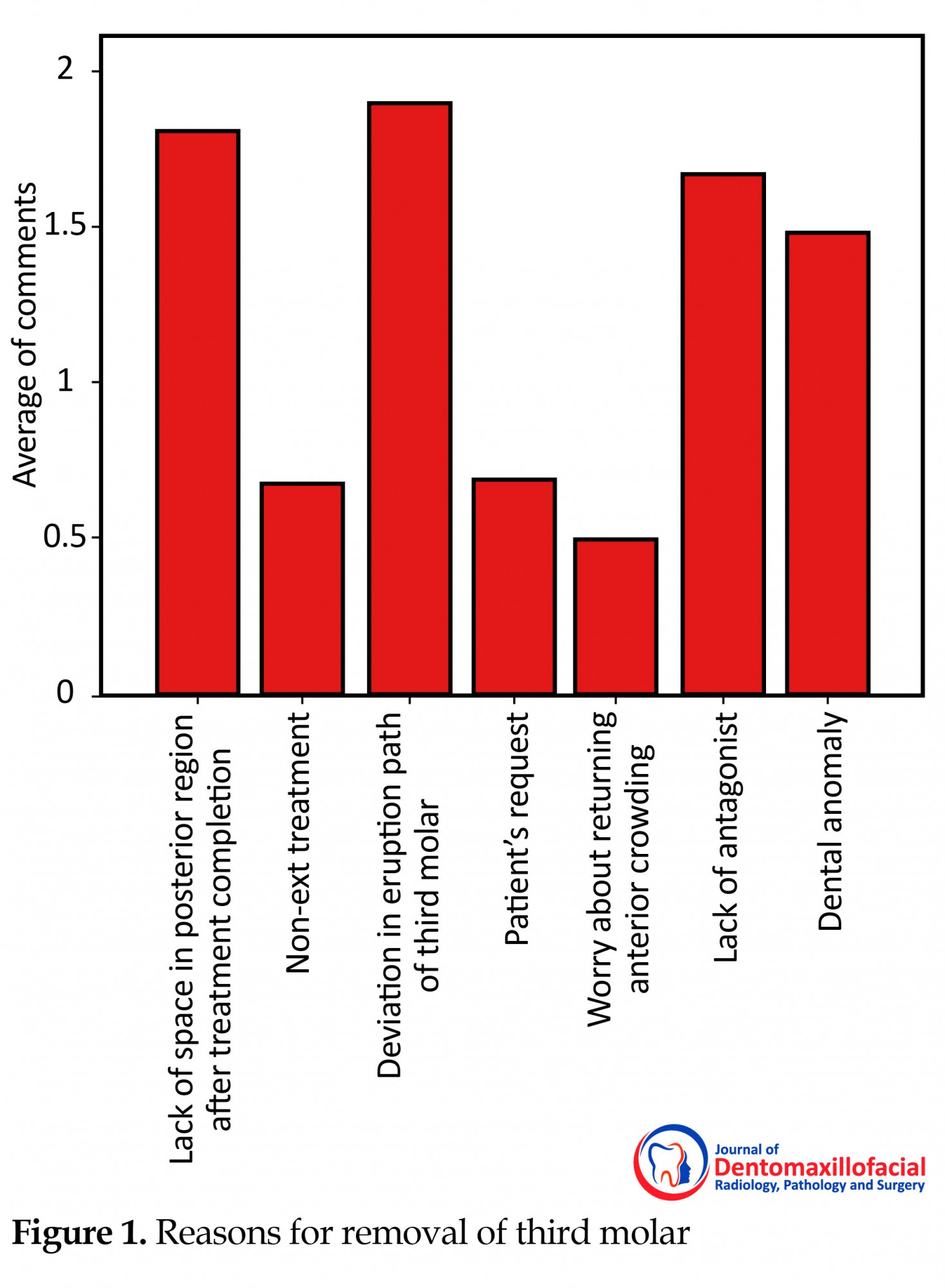
All the samples who belonged in the age group of 30-39 years agreed with the idea of removal of the third molar owning to lack of space. Of the participants who were in favor of removal of the teeth due to lack of space, 91.5% had studied in Iran. According to the answers, the most popular reason for removal of third molar are deviation in eruption path, lack of space in posterior region, and lack of antagonist (Figure 1). We found a positive correlation between the age of the practitioner and tooth removal because of lack of space in posterior region (P=0.014). It means that younger professionals were more in favor of such references. There was also a correlation between the sex of the practitioner and two of the removal reasons- patient’s request (P=0.029) and lack of antagonist (P=0.045). The finding showed that most of the participants (96.2%) disagreed with prophylactic removal to avoid future relapse. We also found a correlation between the place of graduation and lack of space (P=0.001). We didn’t find any correlation between professional practice experience and removal reasons. We also found a correlation between late anterior crowding concern and the seventh and eighth panoramic clichés (P=0.042, P=0.049, respectively).
4. Discussion
The current study aimed to evaluate the opinion of Iranian orthodontists, and the relationship between their decision-making process and some variables as their different cultures, place of graduation, sex and professional practice experience.
In 2009, Eser Tüfekçia et al. [13, 16] compared Swedish orthodontists’ opinions about the role of erupting third molars as a cause of dental crowding with their fellow American orthodontists. They found that most of the American and Swedish orthodontists believe that third molar eruption exerts an anterior force. In spite of this belief, they think that these teeth “rarely” or “never” cause late crowding. In 2007, Steven et al. [14, 10] reported that orthodontists and oral surgeons point of view, mandibular third molars are more likely to cause late crowding and because of that they often remove these teeth prophylactically.
We found that although 21.2% of orthodontists in Iran believe that third molar can cause late crowding but only 3.8% of them referred their patients for prophylactic removal to prevent future relapses. They believe that late crowding concern results in mandibular third molar removal in comparison to maxillary third molar. This finding is consistent with the results of three other studies conducted by Steven et al., Eser Tüfekçia et al., and Snug Jin Kin et al. [13, 14, 16, 10].
This study also showed that the clinicians’ sex and their place of graduation could affect their decision-making. It was indicated that almost every man agreed with the idea of third molar removal if it did not have any antagonist tooth, and most of the men disagreed with prophylactic removal because of patient’s request. About the place of graduation, most clinicians who had studied in Iran, were in agreement with asymptomatic pathologic-free third molar removal and the striking reason was lack of space.
5. Conclusion
According to the answers of Iranian orthodontists, the three most significant reasons for asymptomatic pathology-free third molar removal are deviation in eruption path, lack of space in posterior region, and lack of antagonist. Mandibular third molar is usually extracted to prevent late anterior crowding. Although 21.2% of orthodontists believe that third molar can cause late anterior crowding, only 3.8% of them referred these cases. Variables such as sex and place of graduation affected clinicians’ decision. Out of the study participants, all the male one and all aged between 30 and 39 years were in agreement with third molar removal due to lack of space.
Acknowledgments
This study was designed as a thesis for Doctoral Degree in General Dentistry and all the expenses were paid by the authors themselves.
Conflict of Interest
The authors declared no conflicts of interest.
References
- Garn SM, Lewis AB, Bonne B. Third molar formation and its developmental course. Angle Orthodontist. 1962; 32(4):270-279.
- Richardson ME, Dent M. Some aspects of lower third molar eruption. Angle Orthodontist. 1974; 44(2):141-5. doi: 10.1043/0003-3219(1974)044<0141:SAOLTM>2.0.CO;2
- Rantanen A. The age of eruption of the third molar teeth: a clinical study based on Finnish university students. Acta Odontologica Scandinavica. 1961; 25(Suppl 48):1-86.
- Garcia RI, Chauncey HH. The eruption of third molars in adults: A 10-year longitudinal study. Oral Surgery, Oral Medicine, Oral Pathology. 1989; 68(1):9–13. doi: 10.1016/0030-4220(89)90107-2
- Sewerin I, von Wowern N. A radiographic four-year follow-up study of asymptomatic mandibular third molars in young adults. International Dental Journal. 1990; 40(1):24-30. PMID: 2307524
- Forsberg CM. Tooth size, spacing, and crowding in relation to eruption or impaction of third molars. American Journal of Orthodontics and Dentofacial Orthopedics. 1988; 94(1):57–62. doi: 10.1016/0889-5406(88)90451-9
- NIH consensus development conference for removal of third molars. The Journal of Oral Surgery. 1980; 38(3):235-6. PMID: 6101618
- Lindauer SJ, Laskin DM, Tüfekçi E, Taylor RS, Cushing BJ, Best AM. Orthodontists’ and surgeons’ opinions on the role of third molars as a cause of dental crowding. American Journal of Orthodontics and Dentofacial Orthopedics. 2007; 132(1):43–8. doi: 10.1016/j.ajodo.2005.07.026
- Özeç İ, Hergüner Siso Ş, Taşdemir U, Ezirganli Ş, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. International Journal of Oral and Maxillofacial Surgery. 2009; 38(12):1279–82. doi: 10.1016/j.ijom.2009.07.007
- Kim SJ, Hwang CJ, Park JH, Kim HJ, Yu HS. Surgical removal of asymptomatic impacted third molars: Considerations for orthodontists and oral surgeons. Seminars in Orthodontics. 2016; 22(1):75–83. doi: 10.1053/j.sodo.2015.10.010
- Werkmeister R, Fillies T, Joos U, Smolka K. Relationship between lower wisdom tooth position and cyst development, deep abscess formation and mandibular angle fracture. Journal of Cranio-Maxillofacial Surgery. 2005; 33(3):164–8. doi: 10.1016/j.jcms.2005.01.011
- Mettes TG, Ghaeminia H, Nienhuijs ME, Perry J, van der Sanden WJ, Plasschaert A. Surgical removal versus retention for the management of asymptomatic impacted wisdom teeth. Mettes TG, editor. Cochrane Database of Systematic Reviews. 2012; (6):CD003879. doi: 10.1002/14651858.cd003879.pub3
- Brickley M, Kay E, Shepherd JP, Armstrong RA. Decision Analysis for lower-third-molar Surgery. Medical Decision Making. SAGE Publications; 1995; 15(2):143–51. doi: 10.1177/0272989x9501500207
- Tulloch JFC, Antczak-Bouckoms AA. Decision analysis in the evaluation of clinical strategies for the management of mandibular third molars. Journal of Dental Education. 1987; 51:652-60.
- White RP, Proffit WR. Evaluation and management of asymptomatic third molars: Lack of symptoms does not equate to lack of pathology. American Journal of Orthodontics and Dentofacial Orthopedics. 2011; 140(1):10–6. doi: 10.1016/j.ajodo.2011.05.007
- Tüfekçi E, Svensk D, Kallunki J, Huggare J, Lindauer SJ, Laskin DM. Opinions of American and Swedish Orthodontists about the Role of Erupting Third Molars as a Cause of Dental Crowding. The Angle Orthodontist. The Angle Orthodontist. 2009; 79(6):1139–42. doi: 10.2319/091708-481r.1
Type of Study: Original article |
Subject:
So on
Received: 2017/04/12 | Accepted: 2017/07/19 | Published: 2017/10/1
Received: 2017/04/12 | Accepted: 2017/07/19 | Published: 2017/10/1
References
1. Garn SM, Lewis AB, Bonne B. Third molar formation and its developmental course. Angle Orthodontist. 1962; 32(4):270-279.
2. Richardson ME, Dent M. Some aspects of lower third molar eruption. Angle Orthodontist. 1974; 44(2):141-5. doi: 10.1043/0003-3219(1974)044<0141:SAOLTM>2.0.CO;2
3. Rantanen A. The age of eruption of the third molar teeth: a clinical study based on Finnish university students. Acta Odontologica Scandinavica. 1961; 25(Suppl 48):1-86.
4. Garcia RI, Chauncey HH. The eruption of third molars in adults: A 10-year longitudinal study. Oral Surgery, Oral Medicine, Oral Pathology. 1989; 68(1):9–13. doi: 10.1016/0030-4220(89)90107-2 [DOI:10.1016/0030-4220(89)90107-2]
5. Sewerin I, von Wowern N. A radiographic four-year follow-up study of asymptomatic mandibular third molars in young adults. International Dental Journal. 1990; 40(1):24-30. PMID: 2307524 [PMID]
6. Forsberg CM. Tooth size, spacing, and crowding in relation to eruption or impaction of third molars. American Journal of Orthodontics and Dentofacial Orthopedics. 1988; 94(1):57–62. doi: 10.1016/0889-5406(88)90451-9 [DOI:10.1016/0889-5406(88)90451-9]
7. NIH consensus development conference for removal of third molars. The Journal of Oral Surgery. 1980; 38(3):235-6. PMID: 6101618
8. Lindauer SJ, Laskin DM, Tüfekçi E, Taylor RS, Cushing BJ, Best AM. Orthodontists' and surgeons' opinions on the role of third molars as a cause of dental crowding. American Journal of Orthodontics and Dentofacial Orthopedics. 2007; 132(1):43–8. doi: 10.1016/j.ajodo.2005.07.026 [DOI:10.1016/j.ajodo.2005.07.026]
9. Özeç İ, Hergüner Siso Ş, Taşdemir U, Ezirganli Ş, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. International Journal of Oral and Maxillofacial Surgery. 2009; 38(12):1279–82. doi: 10.1016/j.ijom.2009.07.007 [DOI:10.1016/j.ijom.2009.07.007]
10. Kim SJ, Hwang CJ, Park JH, Kim HJ, Yu HS. Surgical removal of asymptomatic impacted third molars: Considerations for orthodontists and oral surgeons. Seminars in Orthodontics. 2016; 22(1):75–83. doi: 10.1053/j.sodo.2015.10.010 [DOI:10.1053/j.sodo.2015.10.010]
11. Werkmeister R, Fillies T, Joos U, Smolka K. Relationship between lower wisdom tooth position and cyst development, deep abscess formation and mandibular angle fracture. Journal of Cranio-Maxillofacial Surgery. 2005; 33(3):164–8. doi: 10.1016/j.jcms.2005.01.011 [DOI:10.1016/j.jcms.2005.01.011]
12. Mettes TG, Ghaeminia H, Nienhuijs ME, Perry J, van der Sanden WJ, Plasschaert A. Surgical removal versus retention for the management of asymptomatic impacted wisdom teeth. Mettes TG, editor. Cochrane Database of Systematic Reviews. 2012; (6):CD003879. doi: 10.1002/14651858.cd003879.pub3 [DOI:10.1002/14651858.CD003879.pub3]
13. Brickley M, Kay E, Shepherd JP, Armstrong RA. Decision Analysis for lower-third-molar Surgery. Medical Decision Making. SAGE Publications; 1995; 15(2):143–51. doi: 10.1177/0272989x9501500207 [DOI:10.1177/0272989X9501500207]
14. Tulloch JFC, Antczak-Bouckoms AA. Decision analysis in the evaluation of clinical strategies for the management of mandibular third molars. Journal of Dental Education. 1987; 51:652-60. [PMID]
15. White RP, Proffit WR. Evaluation and management of asymptomatic third molars: Lack of symptoms does not equate to lack of pathology. American Journal of Orthodontics and Dentofacial Orthopedics. 2011; 140(1):10–6. doi: 10.1016/j.ajodo.2011.05.007 [DOI:10.1016/j.ajodo.2011.05.007]
16. Tüfekçi E, Svensk D, Kallunki J, Huggare J, Lindauer SJ, Laskin DM. Opinions of American and Swedish Orthodontists about the Role of Erupting Third Molars as a Cause of Dental Crowding. The Angle Orthodontist. The Angle Orthodontist. 2009; 79(6):1139–42. doi: 10.2319/091708-481r.1 [DOI:10.2319/091708-481R.1]
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
