Wed, Apr 24, 2024
Volume 7, Issue 3 (9-2018)
2018, 7(3): 95-102 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Etemadi S, Karbasi kheir M, Khoroushi M. Sensitivity and Specificity of Cone Beam Computed Tomography and Digital Periapical Radiography in Detecting Artificial Buccal Recurrent Caries. Journal title 2018; 7 (3) :95-102
URL: http://3dj.gums.ac.ir/article-1-318-en.html
URL: http://3dj.gums.ac.ir/article-1-318-en.html



1- Assistant Professor, Community Health Research Center, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan, Iran.
2- oral and maxillofacial radiologist, isfahan, iran. , mastoor28@yahoo.com
3- Professor, Dental Material Research Institute, Department of Operative Dentistry, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran.
2- oral and maxillofacial radiologist, isfahan, iran. , mastoor28@yahoo.com
3- Professor, Dental Material Research Institute, Department of Operative Dentistry, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran.
Full-Text [PDF 750 kb]
(639 Downloads)
| Abstract (HTML) (2279 Views)


Full-Text: (1014 Views)
1. Introduction
he term recurrent or secondary caries refers to caries developed at the margin of restorations. Recurrent caries occurs when a restoration is functional for some time and can be detected clinically at gingival margins of all types of class II and V restorations. Recurrent caries results in restorative failure. Thus, it is important to detect recurrent caries at proximal or gingival sites of restorations by radiography providing that the X-rays be at an optimal angle relating to the lesion. However, the radio-opacity of dental materials can hide caries, and their diagnosis by intraoral radiographs depends on the beam angulation, superimposition of anatomical structures, and patient-related factors [1].
Digital intraoral systems include a solid-state silicon chip or a photostimulable Phosphor Storage Plate (PSP). PSP provides a two-dimensional image, which limits the detection of recurrent caries in buccal and lingual or even proximal tooth surfaces [2, 3]. It is difficult to detect buccal recurrent caries under restorations in radiographic examinations. Greater radio-opacity of amalgam restorations compared to enamel can interfere with the detection of lesions in the lingual and buccal areas [3, 4].
Cone Beam Computed Tomography (CBCT) scan is widely used in several dental applications like detecting marginal leakage, vertical root fractures, etc. with a radiation dose lower than Computed Tomography (CT). However, the patient receives a higher dose in CBCT than in intraoral radiographs. Although CBCT provides 3D images, beam hardening, and metal artifacts cause limitations in the detection of recurrent caries under restorations [3-7].
This study aims to compare the validity, sensitivity, and specificity of PSP as the gold standard with CBCT scan in the detection of buccal recurrent caries under amalgam and composite resin restorations.
2. Materials and Methods
A total of 42 extracted human premolars and molars were selected through simple sampling method. The inclusion criterion was the intact crown, and the exclusion criteria were previous restorations and significant caries. The teeth were cleaned of calculus, soft tissue, and debris by hand instrumentation. After surface debridement, they were stored in 0.5% chloramine-T solution in the refrigerator. It took two months to collect the extracted teeth. A class V cavity was prepared on the buccal surface of each tooth using a cylindrical diamond bur, 0.6mm in diameter, (Tizkavan-Iran) mounted on a high-speed headpiece using air-water coolant spray (CH-4T5NSK B2/B3, Japan A1101800). Cavities were 3 mm in width, 1.5 mm in depth, and 2.5 mm in height.
The teeth were randomly divided into two groups of amalgam and composite resin fillings. Twenty-one teeth were filled with amalgam (Sinalux; Dr. Faghihi, Dental Co. Iran). Artificial buccal recurrent caries was simulated on eleven amalgam restored teeth with the aid of a carbide bur (1 mm in diameter). The simulated caries were round cavities with 1mm in width and 1mm in depth, located exactly under the middle of gingival margin of restorations and sealed with 1mm rose wax (Coltène/Whaledent, Switzerland). Ten amalgam restored teeth were left without simulated caries. Twenty-one other teeth were filled with composite resin (GRADIA DIRECT, Posterior, CE0086, Japan) and cured for 40 seconds with 700 mW/cm2 light intensity by an LED light cure (LED Turbo light cure-Taiwan).
Before filling, the cavities were conditioned with SE bond (Lot No. 71167; Kuraray medical Inc. Okayama, Japan) adhesive system. The composite restorative material was placed and condensed incrementally until the preparation was completely filled. Each increment had been light polymerized for 40 seconds before placement of the subsequent increment. Artificial buccal recurrent caries was simulated on ten composite-resin restored teeth with the aid of a carbide bur (1 mm in diameter). The simulated caries were round cavities with 1 mm in width and 1 mm in depth, located precisely under the middle of gingival margin of restorations and sealed with 1 mm rose wax. Eleven composite resin restored teeth were left without simulated caries.
The amalgam and composite resin restored teeth were randomly mounted on two green self-curing acrylic resin arches (green self-cure acrylic resin, Acroparse, Iran). The teeth were placed near each other, in acrylic arches, in the way that each tooth had contact with the adjacent tooth. There was no space between teeth and, similarly, any teeth overlap. CBCT images of each acrylic arch were taken by New Tom VGI (New Tom VGi evo; Quantitative Radiology, Verona, Italy) using a flat panel detector. The adjusted scan parameters were 110 kVp, 3 mA, and 4.3 s. The field of view was 10×5 Hi-Res. and voxel size was 0.15 mm. CBCT projections were analyzed by NNT software in tangential and cross-sectional planes (slice thickness=0.5 mm and slice distance=0.1 mm).
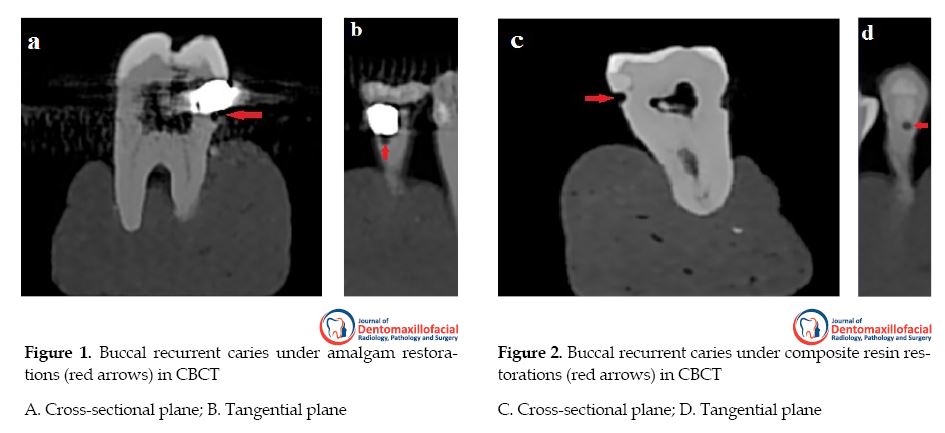
Intraoral periapical digital radiographs were taken by parallel method using a PSP digital intraoral system (Planmeca, Finland) with intraoral radiographic tube (Planmeca, Finland). The adjusted scan parameters were 63 kVp, 8 mA, 0.16 s and 2.6 mm aluminum equivalent filtration. A size tow imaging plate was used, and the exposed phosphor plates were scanned (Scanner Pro, Romexis 351 software, Planmeca, Finland) immediately after exposure. All images were displayed on a 19-inch LG LED monitor (E2042C, Korea) in a room with dim light. No extra adjustment of brightness and contrast was allowed. Figures 1 and 2 show examples of cross-sectional and tangential images obtained by CBCT for amalgam and composite resin restored teeth, and buccal recurrent caries shown by arrows can be detected under each restoration.
he term recurrent or secondary caries refers to caries developed at the margin of restorations. Recurrent caries occurs when a restoration is functional for some time and can be detected clinically at gingival margins of all types of class II and V restorations. Recurrent caries results in restorative failure. Thus, it is important to detect recurrent caries at proximal or gingival sites of restorations by radiography providing that the X-rays be at an optimal angle relating to the lesion. However, the radio-opacity of dental materials can hide caries, and their diagnosis by intraoral radiographs depends on the beam angulation, superimposition of anatomical structures, and patient-related factors [1].
Digital intraoral systems include a solid-state silicon chip or a photostimulable Phosphor Storage Plate (PSP). PSP provides a two-dimensional image, which limits the detection of recurrent caries in buccal and lingual or even proximal tooth surfaces [2, 3]. It is difficult to detect buccal recurrent caries under restorations in radiographic examinations. Greater radio-opacity of amalgam restorations compared to enamel can interfere with the detection of lesions in the lingual and buccal areas [3, 4].
Cone Beam Computed Tomography (CBCT) scan is widely used in several dental applications like detecting marginal leakage, vertical root fractures, etc. with a radiation dose lower than Computed Tomography (CT). However, the patient receives a higher dose in CBCT than in intraoral radiographs. Although CBCT provides 3D images, beam hardening, and metal artifacts cause limitations in the detection of recurrent caries under restorations [3-7].
This study aims to compare the validity, sensitivity, and specificity of PSP as the gold standard with CBCT scan in the detection of buccal recurrent caries under amalgam and composite resin restorations.
2. Materials and Methods
A total of 42 extracted human premolars and molars were selected through simple sampling method. The inclusion criterion was the intact crown, and the exclusion criteria were previous restorations and significant caries. The teeth were cleaned of calculus, soft tissue, and debris by hand instrumentation. After surface debridement, they were stored in 0.5% chloramine-T solution in the refrigerator. It took two months to collect the extracted teeth. A class V cavity was prepared on the buccal surface of each tooth using a cylindrical diamond bur, 0.6mm in diameter, (Tizkavan-Iran) mounted on a high-speed headpiece using air-water coolant spray (CH-4T5NSK B2/B3, Japan A1101800). Cavities were 3 mm in width, 1.5 mm in depth, and 2.5 mm in height.
The teeth were randomly divided into two groups of amalgam and composite resin fillings. Twenty-one teeth were filled with amalgam (Sinalux; Dr. Faghihi, Dental Co. Iran). Artificial buccal recurrent caries was simulated on eleven amalgam restored teeth with the aid of a carbide bur (1 mm in diameter). The simulated caries were round cavities with 1mm in width and 1mm in depth, located exactly under the middle of gingival margin of restorations and sealed with 1mm rose wax (Coltène/Whaledent, Switzerland). Ten amalgam restored teeth were left without simulated caries. Twenty-one other teeth were filled with composite resin (GRADIA DIRECT, Posterior, CE0086, Japan) and cured for 40 seconds with 700 mW/cm2 light intensity by an LED light cure (LED Turbo light cure-Taiwan).
Before filling, the cavities were conditioned with SE bond (Lot No. 71167; Kuraray medical Inc. Okayama, Japan) adhesive system. The composite restorative material was placed and condensed incrementally until the preparation was completely filled. Each increment had been light polymerized for 40 seconds before placement of the subsequent increment. Artificial buccal recurrent caries was simulated on ten composite-resin restored teeth with the aid of a carbide bur (1 mm in diameter). The simulated caries were round cavities with 1 mm in width and 1 mm in depth, located precisely under the middle of gingival margin of restorations and sealed with 1 mm rose wax. Eleven composite resin restored teeth were left without simulated caries.
The amalgam and composite resin restored teeth were randomly mounted on two green self-curing acrylic resin arches (green self-cure acrylic resin, Acroparse, Iran). The teeth were placed near each other, in acrylic arches, in the way that each tooth had contact with the adjacent tooth. There was no space between teeth and, similarly, any teeth overlap. CBCT images of each acrylic arch were taken by New Tom VGI (New Tom VGi evo; Quantitative Radiology, Verona, Italy) using a flat panel detector. The adjusted scan parameters were 110 kVp, 3 mA, and 4.3 s. The field of view was 10×5 Hi-Res. and voxel size was 0.15 mm. CBCT projections were analyzed by NNT software in tangential and cross-sectional planes (slice thickness=0.5 mm and slice distance=0.1 mm).
Intraoral periapical digital radiographs were taken by parallel method using a PSP digital intraoral system (Planmeca, Finland) with intraoral radiographic tube (Planmeca, Finland). The adjusted scan parameters were 63 kVp, 8 mA, 0.16 s and 2.6 mm aluminum equivalent filtration. A size tow imaging plate was used, and the exposed phosphor plates were scanned (Scanner Pro, Romexis 351 software, Planmeca, Finland) immediately after exposure. All images were displayed on a 19-inch LG LED monitor (E2042C, Korea) in a room with dim light. No extra adjustment of brightness and contrast was allowed. Figures 1 and 2 show examples of cross-sectional and tangential images obtained by CBCT for amalgam and composite resin restored teeth, and buccal recurrent caries shown by arrows can be detected under each restoration.
Figure 3 demonstrates the buccal recurrent caries under amalgam, and composite resin restored teeth using PSP digital intraoral system. All the images were viewed and analyzed by two maxillofacial radiologists to detect recurrent caries under the class V restored cavities. The images were arranged in random but were the same for both observers. Since the teeth were placed randomly in the acrylic arches, none of the observers knew that the examined teeth had recurrent caries or not. The observers did not use tangential and cross-sectional planes at the same time.
Statistical analysis
Kappa coefficients were computed to evaluate the inter-observer agreement of the images taken by CBCT and PSP systems. Statistical comparisons were made between the data of CBCT and PSP to assess the agreement between them. Sensitivity and specificity of CBCT and PSP in detecting buccal recurrent caries under amalgam and composite resin restorations were calculated. Statistical significance was set at P-value less than 0.05.
3. Results
The Kappa coefficient for the inter-observer agreement of CBCT projections in tangential plane was 0.829 (P<0.001), for CBCT projections in cross-sectional plane was 0.952 (P<0.001), and for intraoral periapical projections was 0.952 (P<0.001).
Amalgam restorations
The Kappa coefficient for inter-observer agreement of CBCT projections in tangential plane was 0.462 (P=0.012) with 90.5% agreement, for inter-observer agreement of CBCT projections in cross-sectional plane was 0.901 (P<0.0010) with 95.2% agreement and for inter-observer agreement of intraoral periapical projections was 0.897 (P<0.001) with 95.2% agreement.
Composite resin restorations
The Kappa coefficient for the inter-observer agreement of CBCT projections in the tangential plane was 1.00 (P<0.001) with 100% agreement, for inter-observer agreement of CBCT projections in cross-sectional plane, was 1.00 (P<0.001) with 100% agreement, and for inter-observer agreement of intraoral periapical projections was 1.00 (P<0.001) with 100% agreement.
CBCT (tangential plane)
In amalgam restorations, the agreement between CBCT and carious teeth was 52.4% (κ=0.079, P=0.593). In composite resin restorations, the agreement between CBCT and carious teeth was 76.2% (κ=0.512, P=0.007).
CBCT (cross-sectional plane)
In amalgam restorations, the agreement between CBCT and carious teeth was 90.5% (κ=0.811, P<0.001). In composite resin restorations, the agreement between CBCT and carious teeth was 100% (κ=1.00, P<0.001).
Periapical radiograph (PSP digital system)
In amalgam restorations, the agreement between periapical radiographs and carious teeth was 80.9% (κ=0.625, P=0.002). In composite resin restorations, the agreement between periapical radiographs and carious teeth was 95.2% (κ=0.905, P<0.001). Table 1 presents the sensitivity and specificity of CBCT and intraoral radiography in detecting recurrent caries under amalgam and composite resin restorations.
Kappa coefficients were computed to evaluate the inter-observer agreement of the images taken by CBCT and PSP systems. Statistical comparisons were made between the data of CBCT and PSP to assess the agreement between them. Sensitivity and specificity of CBCT and PSP in detecting buccal recurrent caries under amalgam and composite resin restorations were calculated. Statistical significance was set at P-value less than 0.05.
3. Results
The Kappa coefficient for the inter-observer agreement of CBCT projections in tangential plane was 0.829 (P<0.001), for CBCT projections in cross-sectional plane was 0.952 (P<0.001), and for intraoral periapical projections was 0.952 (P<0.001).
Amalgam restorations
The Kappa coefficient for inter-observer agreement of CBCT projections in tangential plane was 0.462 (P=0.012) with 90.5% agreement, for inter-observer agreement of CBCT projections in cross-sectional plane was 0.901 (P<0.0010) with 95.2% agreement and for inter-observer agreement of intraoral periapical projections was 0.897 (P<0.001) with 95.2% agreement.
Composite resin restorations
The Kappa coefficient for the inter-observer agreement of CBCT projections in the tangential plane was 1.00 (P<0.001) with 100% agreement, for inter-observer agreement of CBCT projections in cross-sectional plane, was 1.00 (P<0.001) with 100% agreement, and for inter-observer agreement of intraoral periapical projections was 1.00 (P<0.001) with 100% agreement.
CBCT (tangential plane)
In amalgam restorations, the agreement between CBCT and carious teeth was 52.4% (κ=0.079, P=0.593). In composite resin restorations, the agreement between CBCT and carious teeth was 76.2% (κ=0.512, P=0.007).
CBCT (cross-sectional plane)
In amalgam restorations, the agreement between CBCT and carious teeth was 90.5% (κ=0.811, P<0.001). In composite resin restorations, the agreement between CBCT and carious teeth was 100% (κ=1.00, P<0.001).
Periapical radiograph (PSP digital system)
In amalgam restorations, the agreement between periapical radiographs and carious teeth was 80.9% (κ=0.625, P=0.002). In composite resin restorations, the agreement between periapical radiographs and carious teeth was 95.2% (κ=0.905, P<0.001). Table 1 presents the sensitivity and specificity of CBCT and intraoral radiography in detecting recurrent caries under amalgam and composite resin restorations.
Amalgam restorations
The comparison between the results of periapical radiographs and the tangential plane of CBCT showed 71.4% agreement (κ=0.250, P=0.186). The comparison between the results of periapical radiographs and the cross-sectional plane of CBCT showed 81% agreement (κ=0.600, P=0.005).
Composite resin restorations
The comparison between the results of periapical radiographs and the tangential plane of CBCT showed 71.4% agreement (κ=0.442, P=0.015) and the comparison between the results of periapical radiographs and the cross-sectional plane of CBCT showed 95.2% agreement (κ=0.905, P<0.001).
4. Discussion
CBCT application in dentistry has become widespread because of its potential to show the teeth and surrounding structures in different planes. This study aimed to compare the sensitivity and specificity of CBCT and PSP in detecting buccal recurrent caries under amalgam and composite resin restorations while considering PSP as the gold standard.
Young et al. compared the efficacy of CBCT images and bitewing radiographs in detecting proximal and occlusal caries in teeth without metallic restorations. They concluded that the sensitivity of CBCT in the detection of caries was higher than that of bitewing radiographs taken by a charge-coupled device sensor [8]. Rathore et al. compared the accuracy of CBCT with intraoral radiographs in detecting occlusal caries in teeth without filling and found no difference between these methods in the detection of occlusal caries [9]. In the above studies, beam hardening artifacts had not caused any problem because radiopaque restoration materials were not used. Beam hardening artifacts originate from metallic restorations, implants, and endodontic restorative materials, and are seen as dark and light streaks that project over adjacent teeth and decrease the quality of CBCT images. Dark bands cause the false impression of dental caries that interfere with caries diagnosis. It seems that beam hardening and metal artifacts of amalgam restorations occurring in CBCT images were the limiting factors in the detection of recurrent caries under restorations, especially amalgam restorations, in this study.
As our results showed, the sensitivity of periapical radiographs with PSP in detecting recurrent caries under amalgam and composite resin restoration was higher than that of the tangential plane of CBCT, because of the beam hardening effect. However, our results showed that, despite the beam hardening and metallic artifacts of radiopaque restorations, the detection ability of recurrent caries in CBCT improved using cross-sectional images because cross-sectional planes of CBCT have less structural superimpositions and thus have more clarity.
It was proved that the amount of artifacts of CBCT was dependent on slices thickness and distance. Selecting thinner slices with shorter distances can worsen the effects of artifacts. This study was used a slice thickness of 0.5mm and slice distance of 0.1mm to compare the ability of CBCT with maximum artifacts and digital radiography in detecting recurrent caries. This can be included as one of the limitations of this study, too.
Shahidi et al. compared the accuracy of CBCT and bitewing radiographs with the PSP system in the detection of simulated occlusal secondary caries under amalgam restorations [10]. They concluded that CBCT was more accurate than the PSP system in detecting occlusal recurrent caries. The present study had different results in comparison to Shahidi et al. study because the detection ability of buccal recurrent caries under amalgam and composite resin restorations were compared between CBCT and PSP systems. Besides, the images of tangential and cross-sectional planes of CBCT were compared with PSP images, separately.
Our results showed that the sensitivity of PSP and cross-sectional plane of CBCT in detecting buccal recurrent caries under composite resin restorations was similar, and the sensitivity of cross-sectional plane of CBCT was higher than PSP in detecting buccal recurrent caries under amalgam restorations. However, the sensitivity of the tangential plane of CBCT is lower than PSP in detecting buccal recurrent caries under amalgam and composite resin restorations.
Some studies have compared the ability of CBCT, CCD, and PSP or film in the detection of caries on proximal or occlusal surfaces; however, there are not many similar studies that compare the ability of CBCT and PSP systems in detection of buccal recurrent caries [5, 11, 12]. The only research covering this subject belongs to Murat et al. who compared CBCT and intraoral radiography in detecting buccal recurrent caries under different types of restorations.
Murat et al. concluded that CBCT was superior to intraoral radiographs in detecting buccal recurrent caries because of the possibility of observing the teeth in different planes. The present study is similar to their work because of using CBCT and intraoral radiography in detecting buccal recurrent caries under amalgam and composite resin restorations [3]. The discrepancy between our results and Murat et al. results can be because of the differences between the CBCT using devices, which have different voxel sizes and artifact reduction software.
The present study supports some aspects of their idea and shows that, in spite of the restorative material, the sensitivity of CBCT in detecting buccal recurrent caries is higher in cross-sectional planes than in tangential planes. Also, our results show that the sensitivity of cross-sectional images and periapical radiographs is equal in the detection of buccal recurrent caries under composite resin restorations. But, under amalgam restorations, the sensitivity of cross-sectional images in the detection of recurrent caries is a little higher than periapical radiographs.
Although CBCT emits a rather low dose of radiation than CT, its exposure dose is still higher than intraoral radiographs with PSPs. The small field of view of CBCT systems results in the lower effective dose and makes it less applicable in detection of caries [13-15]. Considering the higher price and exposure dose of CBCT, PSP systems can still be recommended for detecting buccal recurrent caries.
In the present study, recurrent caries was created by a carbide bur (1 mm in diameter). Thus, the artificial recurrent caries was well-defined [5, 10]. The well-defined border helps the examiners to differentiate recurrent caries from adjacent superimposed structures and to detect recurrent caries, especially in the PSP system. However, true recurrent caries is not somehow well-defined, and this may cause misinterpretation in true recurrent caries which may be considered as anther limitation of this research.
For future studies, it is suggested to use the teeth with true buccal recurrent caries for the differentiation of the ability of PSP and CBCT. In this study, the sensitivity of CBCT and PSP system in detecting buccal recurrent caries under composite resin restorations was more than that of amalgam restorations. On the other hand, the observers performed better when assessing buccal recurrent caries under composite restorations than under amalgam ones. This finding agrees with another study using CBCT to detect occlusal and proximal recurrent caries under amalgam and composite restorations [12].
Although clinical examinations play an essential role in the detection of buccal recurrent caries, this study only compared the ability of two radiographic systems in the detection of buccal recurrent caries under amalgam and composite resin restorations; that is, findings of clinical examination have been overlooked in this research.
5. Conclusion
Considering the limitations of the study, we conclude that the sensitivity of CBCT in different planes is more than that of intraoral radiography with the PSP system, and the cross-sectional plan has a higher sensitivity than a tangential plane in the detection of recurrent caries. However, because of equal sensitivity of cross-sectional images of CBCT and PSP in detection of recurrent caries under composite resin restorations and approximate equality of cross-sectional images of CBCT and PSP in the detection of recurrent caries under amalgam restorations, intraoral radiography with PSP system remains a rival for CBCT in detecting buccal recurrent caries.
Ethical Considerations
Compliance with ethical guidelines
There was no ethical considerations to be considered in this research.
Funding
This study was part of a research project (Grant No: 295258) supported and funded by Isfahan University of Medical Sciences.
Authors contribution's
Conceptualization: Maryam Khoroushi; Methodology, software, validation, formal analysis, investigation, resources, data curation: Mitra Karbasi kheir, Maryam Khoroushi; Writing-original draft preparation, writing-review & editing: Mitra Karbasi kheir, Maryam Khoroushi; Visualization, supervision, project administration, funding acquisition: Maryam Khoroushi, Shahab Etemadi.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this paper, except, the first and second authors contributed equally to this manuscript and are considered as first co-authors.
Acknowledgements
The authors would like to appreciate the Research Center of Shool of Dentistry of the Isfahan University of Medical Sciences for supporting this study.
References
The comparison between the results of periapical radiographs and the tangential plane of CBCT showed 71.4% agreement (κ=0.250, P=0.186). The comparison between the results of periapical radiographs and the cross-sectional plane of CBCT showed 81% agreement (κ=0.600, P=0.005).
Composite resin restorations
The comparison between the results of periapical radiographs and the tangential plane of CBCT showed 71.4% agreement (κ=0.442, P=0.015) and the comparison between the results of periapical radiographs and the cross-sectional plane of CBCT showed 95.2% agreement (κ=0.905, P<0.001).
4. Discussion
CBCT application in dentistry has become widespread because of its potential to show the teeth and surrounding structures in different planes. This study aimed to compare the sensitivity and specificity of CBCT and PSP in detecting buccal recurrent caries under amalgam and composite resin restorations while considering PSP as the gold standard.
Young et al. compared the efficacy of CBCT images and bitewing radiographs in detecting proximal and occlusal caries in teeth without metallic restorations. They concluded that the sensitivity of CBCT in the detection of caries was higher than that of bitewing radiographs taken by a charge-coupled device sensor [8]. Rathore et al. compared the accuracy of CBCT with intraoral radiographs in detecting occlusal caries in teeth without filling and found no difference between these methods in the detection of occlusal caries [9]. In the above studies, beam hardening artifacts had not caused any problem because radiopaque restoration materials were not used. Beam hardening artifacts originate from metallic restorations, implants, and endodontic restorative materials, and are seen as dark and light streaks that project over adjacent teeth and decrease the quality of CBCT images. Dark bands cause the false impression of dental caries that interfere with caries diagnosis. It seems that beam hardening and metal artifacts of amalgam restorations occurring in CBCT images were the limiting factors in the detection of recurrent caries under restorations, especially amalgam restorations, in this study.
As our results showed, the sensitivity of periapical radiographs with PSP in detecting recurrent caries under amalgam and composite resin restoration was higher than that of the tangential plane of CBCT, because of the beam hardening effect. However, our results showed that, despite the beam hardening and metallic artifacts of radiopaque restorations, the detection ability of recurrent caries in CBCT improved using cross-sectional images because cross-sectional planes of CBCT have less structural superimpositions and thus have more clarity.
It was proved that the amount of artifacts of CBCT was dependent on slices thickness and distance. Selecting thinner slices with shorter distances can worsen the effects of artifacts. This study was used a slice thickness of 0.5mm and slice distance of 0.1mm to compare the ability of CBCT with maximum artifacts and digital radiography in detecting recurrent caries. This can be included as one of the limitations of this study, too.
Shahidi et al. compared the accuracy of CBCT and bitewing radiographs with the PSP system in the detection of simulated occlusal secondary caries under amalgam restorations [10]. They concluded that CBCT was more accurate than the PSP system in detecting occlusal recurrent caries. The present study had different results in comparison to Shahidi et al. study because the detection ability of buccal recurrent caries under amalgam and composite resin restorations were compared between CBCT and PSP systems. Besides, the images of tangential and cross-sectional planes of CBCT were compared with PSP images, separately.
Our results showed that the sensitivity of PSP and cross-sectional plane of CBCT in detecting buccal recurrent caries under composite resin restorations was similar, and the sensitivity of cross-sectional plane of CBCT was higher than PSP in detecting buccal recurrent caries under amalgam restorations. However, the sensitivity of the tangential plane of CBCT is lower than PSP in detecting buccal recurrent caries under amalgam and composite resin restorations.
Some studies have compared the ability of CBCT, CCD, and PSP or film in the detection of caries on proximal or occlusal surfaces; however, there are not many similar studies that compare the ability of CBCT and PSP systems in detection of buccal recurrent caries [5, 11, 12]. The only research covering this subject belongs to Murat et al. who compared CBCT and intraoral radiography in detecting buccal recurrent caries under different types of restorations.
Murat et al. concluded that CBCT was superior to intraoral radiographs in detecting buccal recurrent caries because of the possibility of observing the teeth in different planes. The present study is similar to their work because of using CBCT and intraoral radiography in detecting buccal recurrent caries under amalgam and composite resin restorations [3]. The discrepancy between our results and Murat et al. results can be because of the differences between the CBCT using devices, which have different voxel sizes and artifact reduction software.
The present study supports some aspects of their idea and shows that, in spite of the restorative material, the sensitivity of CBCT in detecting buccal recurrent caries is higher in cross-sectional planes than in tangential planes. Also, our results show that the sensitivity of cross-sectional images and periapical radiographs is equal in the detection of buccal recurrent caries under composite resin restorations. But, under amalgam restorations, the sensitivity of cross-sectional images in the detection of recurrent caries is a little higher than periapical radiographs.
Although CBCT emits a rather low dose of radiation than CT, its exposure dose is still higher than intraoral radiographs with PSPs. The small field of view of CBCT systems results in the lower effective dose and makes it less applicable in detection of caries [13-15]. Considering the higher price and exposure dose of CBCT, PSP systems can still be recommended for detecting buccal recurrent caries.
In the present study, recurrent caries was created by a carbide bur (1 mm in diameter). Thus, the artificial recurrent caries was well-defined [5, 10]. The well-defined border helps the examiners to differentiate recurrent caries from adjacent superimposed structures and to detect recurrent caries, especially in the PSP system. However, true recurrent caries is not somehow well-defined, and this may cause misinterpretation in true recurrent caries which may be considered as anther limitation of this research.
For future studies, it is suggested to use the teeth with true buccal recurrent caries for the differentiation of the ability of PSP and CBCT. In this study, the sensitivity of CBCT and PSP system in detecting buccal recurrent caries under composite resin restorations was more than that of amalgam restorations. On the other hand, the observers performed better when assessing buccal recurrent caries under composite restorations than under amalgam ones. This finding agrees with another study using CBCT to detect occlusal and proximal recurrent caries under amalgam and composite restorations [12].
Although clinical examinations play an essential role in the detection of buccal recurrent caries, this study only compared the ability of two radiographic systems in the detection of buccal recurrent caries under amalgam and composite resin restorations; that is, findings of clinical examination have been overlooked in this research.
5. Conclusion
Considering the limitations of the study, we conclude that the sensitivity of CBCT in different planes is more than that of intraoral radiography with the PSP system, and the cross-sectional plan has a higher sensitivity than a tangential plane in the detection of recurrent caries. However, because of equal sensitivity of cross-sectional images of CBCT and PSP in detection of recurrent caries under composite resin restorations and approximate equality of cross-sectional images of CBCT and PSP in the detection of recurrent caries under amalgam restorations, intraoral radiography with PSP system remains a rival for CBCT in detecting buccal recurrent caries.
Ethical Considerations
Compliance with ethical guidelines
There was no ethical considerations to be considered in this research.
Funding
This study was part of a research project (Grant No: 295258) supported and funded by Isfahan University of Medical Sciences.
Authors contribution's
Conceptualization: Maryam Khoroushi; Methodology, software, validation, formal analysis, investigation, resources, data curation: Mitra Karbasi kheir, Maryam Khoroushi; Writing-original draft preparation, writing-review & editing: Mitra Karbasi kheir, Maryam Khoroushi; Visualization, supervision, project administration, funding acquisition: Maryam Khoroushi, Shahab Etemadi.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this paper, except, the first and second authors contributed equally to this manuscript and are considered as first co-authors.
Acknowledgements
The authors would like to appreciate the Research Center of Shool of Dentistry of the Isfahan University of Medical Sciences for supporting this study.
References
- Mjör I. Clinical diagnosis of recurrent caries. Journal of the American Dental Association (JADA) 2005; 136(10):1426-33. [DOI:10.14219/jada.archive.2005.0057] [PMID]
- Hildebolt CF, Couture RA, Whiting BR. Dental photostimulable phosphor radiography. Dental Clinics of North America. 2000; 44(2):273-97.
- Murat S, Kamburoğlu K, Isayev A, Kurşun S, Yüksel S. Visibility of artificial buccal recurrent caries under restorations using different radiographic techniques. Operative Dentistry. 2013; 38(2):197-207. [DOI:10.2341/12-158-L] [PMID]
- Kandemir S. The radiographic investigation of the visibility of secondary caries adjacent to the gingiva in Class II amalgam restorations. Quintessence International. 1997; 28(6): 387-92. [PMID]
- Charuakkra A, Prapayasatok S, Janhom A, Pongsiriwet S, Verochana K, Mahasantipiya Ph. Diagnostic performance of Cone-Beam Computed Tomography on detection of mechanically-created artificial secondary caries. Imaging Science in Dentistry. 2011; 41(4):143-50. [DOI:10.5624/isd.2011.41.4.143] [PMID] [PMCID]
- Khoroushi M, Etemadi S, Karbasi Kheir M. Marginal leakage of Class V composite resin restoations. Dental Hypotheses. 2018; 9(1):11-5.
- Hekmatian E, Karbasi Kheir M, Fathollahzade H, Sheikhi M. Detection of vertical root fractures using cone-beam computed tomography in the presence and absence of Gutta-Percha. The Scientific World Journal. 2018:1-5. [DOI: 10.1155/2018/1920946]
- Young SM, Lee JT, Hodges RJ, Chang T-L, Elashoff DA, White SC. A comparative study of high-resolution Cone Beam Computed Tomography and charge-coupled device sensors for detecting caries. Dento Maxillo Facial Radiology. 2009; 38(7):445-51. [DOI:10.1259/dmfr/88765582] [PMID]
- Rathore S, Tyndall D, Wright JT, Everett E. Ex vivo comparison of Galileos Cone Beam CT and intraoral radiographs in detecting occlusal caries. Dento Maxillo Facial Radiology. 2012; 41(6):489-93. [DOI:10.1259/dmfr/57329547] [PMID] [PMCID]
- Shahidi Sh, Kazerooni Zadeh N, Sharafeddin F, Shahab Sh, Bahrampour E, Hamedani Sh. An in vitro comparison of diagnostic accuracy of Cone Beam Computed Tomography and phosphor storage plate to detect simulated occlusal secondary caries under amalgam restoration. Dental Research Journal. 2015; 12(2):161-6. [PMID] [PMCID]
- Akdeniz BG, Gröndahl HG, Magnusson B. Accuracy of proximal caries depth measurements: Comparison between limited Cone Beam Computed Tomography, storage phosphor and film radiography. Caries Research. 2006; 40(3):202-7. [DOI:10.1159/000092226] [PMID]
- Baltacıoĝlu İH, Eren H, Yavuz Y, Kamburoğlu K. Diagnostic accuracy of different display types in detection of recurrent caries under restorations by using CBCT. Dento Maxillo Facial Radiology. 2016; 45(6):20160099. [DOI:10.1259/dmfr.20160099] [PMID] [PMCID]
- Ludlow JB, Ludlow LED, Brooks SL, Howerton WB. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercury, NewTom 3G, and i-CAT. Dento Maxillo Facial Radiology. 2006; 35(4):219-26. [DOI:10.1259/dmfr/14340323] [PMID]
- Hirsch E, Wolf U, Heinicke F, Silva MA. Dosimetry of the Cone Beam Computed Tomography Veraviewepocs 3D compared with the 3D Accuitomo indifferent field of views. Dento maxillofacial radiology. 2008; 37(5):268-73. [DOI:10.1259/dmfr/23424132] [PMID]
- Ludlow JB, Davies-Ludlow LE, White SC. Patient risk related to common dental radiographic examinations: The impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculation. Journal of the American Dental Association. 2008; 139(9): 1237-43. [DOI:10.14219/jada.archive.2008.0339] [PMID]
Type of Study: Original article |
Subject:
Radiology
Received: 2018/01/10 | Accepted: 2018/07/23 | Published: 2018/09/1
Received: 2018/01/10 | Accepted: 2018/07/23 | Published: 2018/09/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
