Thu, Apr 25, 2024
Volume 6, Issue 3 (10-2017)
2017, 6(3): 77-82 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Taramsari M, Dalili Kajan Z, Atash Biz Yeganeh L. An Oculofaciocardiodental Syndrome: Challenges in Endodontic Treatment. Journal title 2017; 6 (3) :77-82
URL: http://3dj.gums.ac.ir/article-1-283-en.html
URL: http://3dj.gums.ac.ir/article-1-283-en.html


1- Associate Professor, Department of Endodontic, Faculty of Dental, Guilan University of Medical Sciences, Rasht, Iran.
2- Professor of Maxillofacial Radiology, Department of Maxillofacial Radiology, Faculty of Dental, Guilan University of Medical Sciences, Rasht, Iran.
3- Assistant Professor, Department of Endodontic, Faculty of Dental, Guilan University of Medical Sciences, Rasht, Iran. , yeganehdds@gmail.com
2- Professor of Maxillofacial Radiology, Department of Maxillofacial Radiology, Faculty of Dental, Guilan University of Medical Sciences, Rasht, Iran.
3- Assistant Professor, Department of Endodontic, Faculty of Dental, Guilan University of Medical Sciences, Rasht, Iran. , yeganehdds@gmail.com
Full-Text [PDF 1684 kb]
(1574 Downloads)
| Abstract (HTML) (3381 Views)



Full-Text: (2190 Views)
1. Case Report
The patient, an 18-year-old female with chief complaint of severe anterior crossbite and chin protrusion, was referred to the orthodontic department of faculty of dentistry of Guilan University medical sciences. In dental exam, due toa periapicallesion associated with maxillary right central incisor, the patient was referred to an endodontist.
In past medical history, unilateral congenital cataracts and mitral valve prolapse were found. She had normal mental maturity. She had no cleft lip or palate and no hearing loss. The patient reported that there were no ocular, cardiologic, dental or abnormal skeletal symptoms apparent in her family.
On clinical examination, she had a long narrow face with broad nasal tip, slight asymmetry and chin protrusion (Figure 1a, b). The other dental findings were angle class III molar relationship, severe anterior crossbite and a constricted maxillary dental arch (Figure 1c, d).
The patient, an 18-year-old female with chief complaint of severe anterior crossbite and chin protrusion, was referred to the orthodontic department of faculty of dentistry of Guilan University medical sciences. In dental exam, due toa periapicallesion associated with maxillary right central incisor, the patient was referred to an endodontist.
In past medical history, unilateral congenital cataracts and mitral valve prolapse were found. She had normal mental maturity. She had no cleft lip or palate and no hearing loss. The patient reported that there were no ocular, cardiologic, dental or abnormal skeletal symptoms apparent in her family.
On clinical examination, she had a long narrow face with broad nasal tip, slight asymmetry and chin protrusion (Figure 1a, b). The other dental findings were angle class III molar relationship, severe anterior crossbite and a constricted maxillary dental arch (Figure 1c, d).
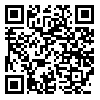
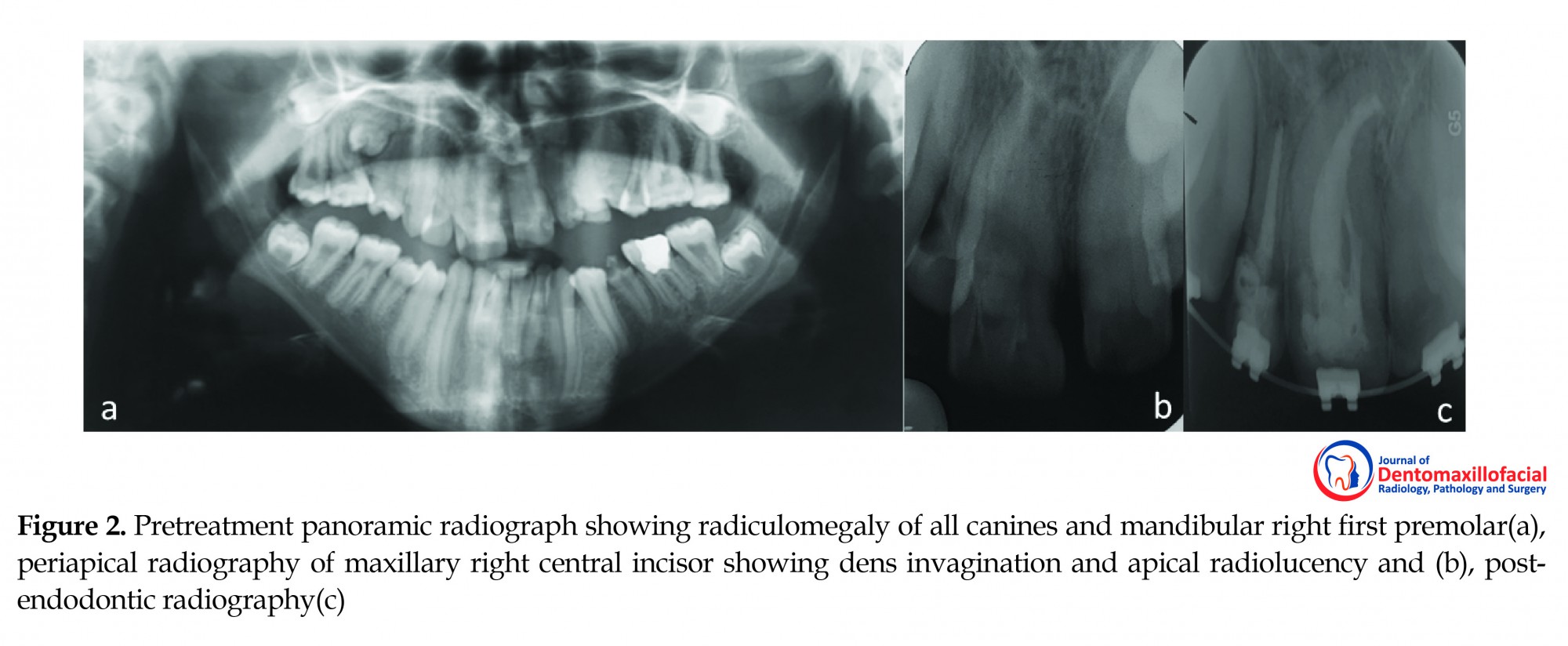
On radiographic examination, delayed loss of primary dentition (primary maxillary left canine), delayed eruption of permanent teeth,impacted permanent teeth (maxillary third molars and right second premolar), and the missing of maxillary left lateral incisor were found. Enamel dysplasia was found on left primary maxillary canine. Canines had very large roots (radiculomegaly). Mandibular right first premolar and maxillary central incisors also had radiculomegaly (Figure 2a). CBCT was obtained and it showed long and curved root canal of canines and apical closure (Figure 3).
Clinical examination revealed a carious lesion in the maxillary right central incisor. The tooth has not normal vitality tests. There was no tenderness on percussion. The diagnosis of pulpal necrosis and chronic apical periodontitis was made. Interpretation of radiography revealed the presence of anomaly in crown-root size, morphology and dens invagination type II Ohler (Figure 2b).
The tooth was anaesthetized with lidocaine 2% containing 1:100000 epinephrine (Daroupakhsh, Tehran, Iran) and isolated with rubber dam. The carious lesion was removed and access cavity was made. A large orifice was apparent, and mesial to the main orifice, there was a smaller orifice, indicated the other root canal. The working length of the main and accessory canals was 28 and 20 mm, respectively, which were merged together at the apical third. After enlarging the orifices with Gates-Glidden burs #1, 2 (DentsplyMaillefer, Ballaigues, Switzerland), the root canals were prepared using hand K-files and RaCe rotary system (FKG Dentaire, La-chaux de-Fonds, Switzerland) and RC Prep (Premier, Norristown, PA, USA) as a lubricant. The last file inserted in each root canal was RaCe rotary file size 50, .04 taper (31 mm). For irrigation, an ultrasonic device was attached to a size 20 K-file inserted in each canal filled with sodium hypochlorite solution (2.5%). The canals were dried with paper points, and obturated with laterally condensed gutta-percha and AH 26 sealer (DentsplyMaillefer, Ballaigues, Switzerland). Finally, the tooth was restored with composite (Figure 2c).
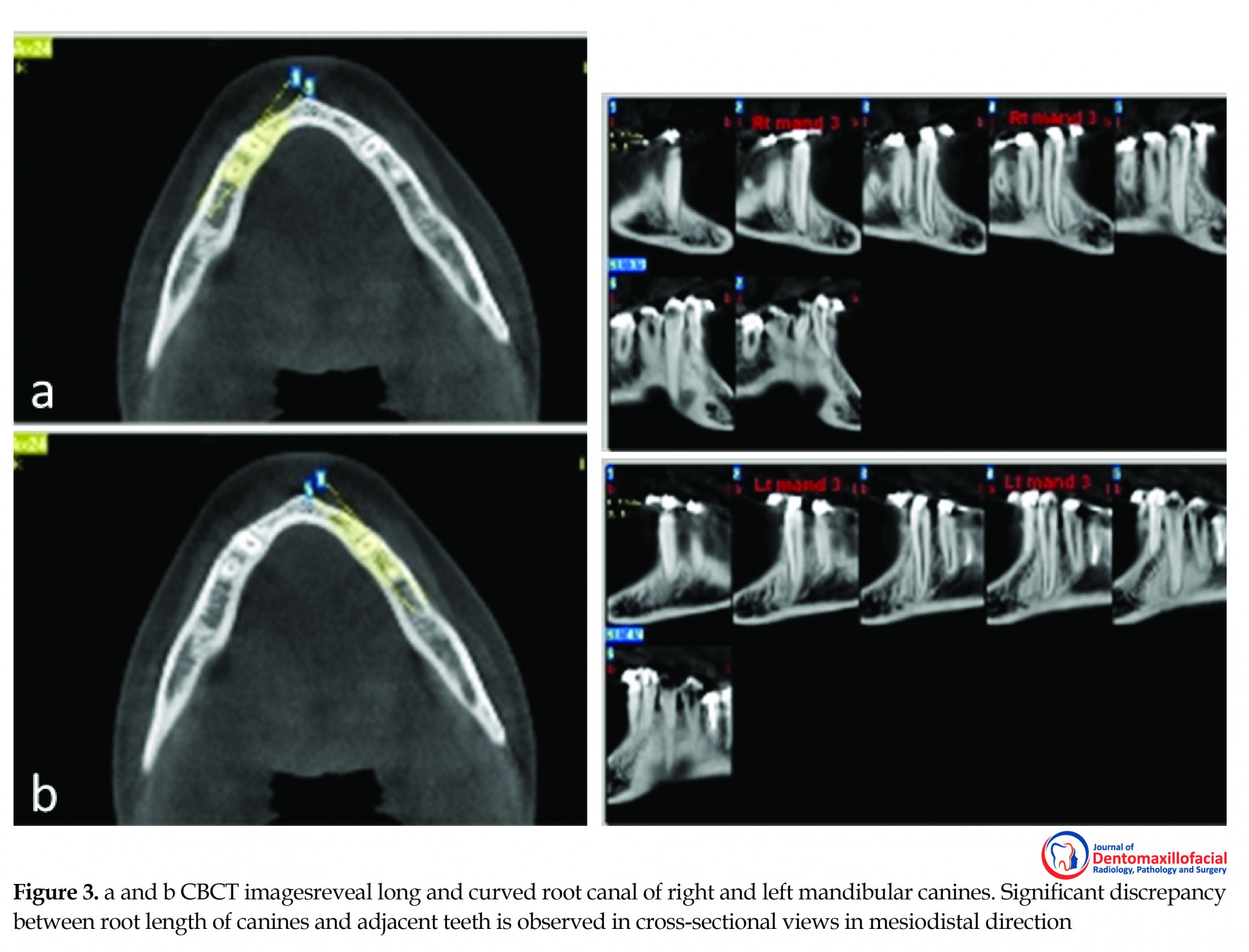
The patient need surgical orthodontics and her orthosurgeon asked us to intentionally treat root canals of mandibular canines to avoid side effects of the surgical process. Estimated working length was at least 35 mm, which make the treatment with conventional instruments impossible. We made a longer file by cutting and removing the handle of each 31 mm length K-file and another file at the initiation of flutes (keeping the handle). And then, these two parts were attached together by soldering (Figure 4a).
The tooth was anaesthetized with lidocaine 2% containing 1:100000 epinephrine (Daroupakhsh, Tehran, Iran) and isolated with rubber dam. The carious lesion was removed and access cavity was made. A large orifice was apparent, and mesial to the main orifice, there was a smaller orifice, indicated the other root canal. The working length of the main and accessory canals was 28 and 20 mm, respectively, which were merged together at the apical third. After enlarging the orifices with Gates-Glidden burs #1, 2 (DentsplyMaillefer, Ballaigues, Switzerland), the root canals were prepared using hand K-files and RaCe rotary system (FKG Dentaire, La-chaux de-Fonds, Switzerland) and RC Prep (Premier, Norristown, PA, USA) as a lubricant. The last file inserted in each root canal was RaCe rotary file size 50, .04 taper (31 mm). For irrigation, an ultrasonic device was attached to a size 20 K-file inserted in each canal filled with sodium hypochlorite solution (2.5%). The canals were dried with paper points, and obturated with laterally condensed gutta-percha and AH 26 sealer (DentsplyMaillefer, Ballaigues, Switzerland). Finally, the tooth was restored with composite (Figure 2c).
The patient need surgical orthodontics and her orthosurgeon asked us to intentionally treat root canals of mandibular canines to avoid side effects of the surgical process. Estimated working length was at least 35 mm, which make the treatment with conventional instruments impossible. We made a longer file by cutting and removing the handle of each 31 mm length K-file and another file at the initiation of flutes (keeping the handle). And then, these two parts were attached together by soldering (Figure 4a).
Access cavities of canines were prepared larger than normal to let the new fabricated files (which had a bigger and brittle shank) enter into the canal. Working length was confirmed at 38 mm by radiography. Apical foramen was opened laterally. Cleaning and shaping of root canals with new designed long hand files using crown-down technique. For choosing the master apical cone, we attached the first 15 mm of the apical portion of gutta-percha (#40) to a bigger guttapercha by rolling them between two glass slabs and creating frictional heat (Figure 4b). A longer spreader was made by the same technique which described for hand K-files (Figure 4c). The canals were obturated with laterally condensed gutta-percha and AH 26 sealer (DentsplyMaillefer, Ballaigues, Switzerland). Finally, the access cavities were restored with composite (Figure 5). 24 months later the patient was symptom free and a radiographic control revealed a continuous periodontal space with no signs of periapical abnormal radiographic changes (Figure 6).
2. Discussion
OFCD syndrome is an X-linked condition which characterized by ocular, facial, cardiac, and dental abnormalities [1]. Hayward was the first who notice dental anomalies in these patients. The main characteristics of OFCD includes microphthalmia, congenital cataracts, large narrow face, deep set eyes, as well as cardiac symptoms such as atrial and/or ventricular defects or mitral valve prolapse [1]. Dental anomalies include radiculomegaly of canines, incisors and somehow premolars, missing teeth, delayed tooth eruption, prolonged retention of primary teeth, as well as enamel and dentine defects [2].dental anomalies are the most important findings, and radiculomegaly of canines is a characteristic criteria for the diagnosis of OFCD syndrome [3]. A mutation in the BCOR gene is considered the cause of the syndrome [4], however DNA sample was not obtained from our patient. She had not been diagnosed with OFCD prior to her visit in our dental clinic at age 18. In our patient, radiculomegaly was observed in the bilateral canines of both dental arches and central maxillary incisors and mandibular right first premolar.
Considering the other anomalies, such as unilateral congenital cataracts, a facial anomaly, such as a long and narrow face, and a cardiac anomaly, such as mitral valve prolapse, this patient was diagnosed with OFCD syndrome. Although open apices of canines and first premolars have been reported in most previous patients [5, 6], it was not found in our patient. Macrodontia and dens invagination of maxillary right central incisor was evident in our patient which was not yet reported for OFCD syndromes.
The prevalence of macrodontia has been estimated to be 0.2%-1.37%, [7, 8] cases of nonsyndromicradiculomegaly are rare as only twenty cases have been documented as at 2010 [5]. Endodontic management of giant roots is difficult. Our patient has a root canal length of canines 38 mm. Pace et al. [6] reported retreatment of an open apex mandibular canine with K-reamer veterinary instrument using crown-down technique. Working length was 40 mm. They used longterm calcium hydroxide therapy for 6 months and obturation was done by modified- thermafil technique. A study by Maden et al. [5] reported endodontic treatment of a canine with radiculomegaly and having two root canals, root dilacerations, increased root length, and open apices. They used vetinox veterinary files (40, 60 mm) with crown-down technique. Working length was 47.5. The apexification procedure was done for 11 months. They used custom-made thermoplastisized gutta-percha in an acrylic mold and obturated the canals with system B continiuos wave compaction technique.
Larhant et al. [9] reported a case of OFCD syndrome that had acute cellulitis and abscess developing from the right mandibular canine. They choose to extract the casual tooth. Histological assessment of the extracted canine (42.5 mm) revealed dentine abnormalities, open apex, disorganized dentine deposition, pulp stones and thin enamel. Devitalization has even been proposed as a preventive procedure for radiculomegaly, and subsequently for its consequences such as increase in vertical dimension [5].
3. Conclusion
This report exemplifies the important role of dentists in recognizing rare syndromic disorders with typical or unusual dental or intraoral phenotypes. Caries prevention and treatment is crucial due to the presence of cardiac malformations in OFCDS. Specific endodontic techniques have to be applied due to root length and open apices.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declared no conflicts of interest.
References
OFCD syndrome is an X-linked condition which characterized by ocular, facial, cardiac, and dental abnormalities [1]. Hayward was the first who notice dental anomalies in these patients. The main characteristics of OFCD includes microphthalmia, congenital cataracts, large narrow face, deep set eyes, as well as cardiac symptoms such as atrial and/or ventricular defects or mitral valve prolapse [1]. Dental anomalies include radiculomegaly of canines, incisors and somehow premolars, missing teeth, delayed tooth eruption, prolonged retention of primary teeth, as well as enamel and dentine defects [2].dental anomalies are the most important findings, and radiculomegaly of canines is a characteristic criteria for the diagnosis of OFCD syndrome [3]. A mutation in the BCOR gene is considered the cause of the syndrome [4], however DNA sample was not obtained from our patient. She had not been diagnosed with OFCD prior to her visit in our dental clinic at age 18. In our patient, radiculomegaly was observed in the bilateral canines of both dental arches and central maxillary incisors and mandibular right first premolar.
Considering the other anomalies, such as unilateral congenital cataracts, a facial anomaly, such as a long and narrow face, and a cardiac anomaly, such as mitral valve prolapse, this patient was diagnosed with OFCD syndrome. Although open apices of canines and first premolars have been reported in most previous patients [5, 6], it was not found in our patient. Macrodontia and dens invagination of maxillary right central incisor was evident in our patient which was not yet reported for OFCD syndromes.
The prevalence of macrodontia has been estimated to be 0.2%-1.37%, [7, 8] cases of nonsyndromicradiculomegaly are rare as only twenty cases have been documented as at 2010 [5]. Endodontic management of giant roots is difficult. Our patient has a root canal length of canines 38 mm. Pace et al. [6] reported retreatment of an open apex mandibular canine with K-reamer veterinary instrument using crown-down technique. Working length was 40 mm. They used longterm calcium hydroxide therapy for 6 months and obturation was done by modified- thermafil technique. A study by Maden et al. [5] reported endodontic treatment of a canine with radiculomegaly and having two root canals, root dilacerations, increased root length, and open apices. They used vetinox veterinary files (40, 60 mm) with crown-down technique. Working length was 47.5. The apexification procedure was done for 11 months. They used custom-made thermoplastisized gutta-percha in an acrylic mold and obturated the canals with system B continiuos wave compaction technique.
Larhant et al. [9] reported a case of OFCD syndrome that had acute cellulitis and abscess developing from the right mandibular canine. They choose to extract the casual tooth. Histological assessment of the extracted canine (42.5 mm) revealed dentine abnormalities, open apex, disorganized dentine deposition, pulp stones and thin enamel. Devitalization has even been proposed as a preventive procedure for radiculomegaly, and subsequently for its consequences such as increase in vertical dimension [5].
3. Conclusion
This report exemplifies the important role of dentists in recognizing rare syndromic disorders with typical or unusual dental or intraoral phenotypes. Caries prevention and treatment is crucial due to the presence of cardiac malformations in OFCDS. Specific endodontic techniques have to be applied due to root length and open apices.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declared no conflicts of interest.
References
- Hayward JR. Cuspid gigantism. Oral Surgery, Oral Medicine, Oral Pathology. 1980; 49(6):500–1. doi: 10.1016/0030-4220(80)90070-5
- Gorlin RJ, Marashi AH, Obwegeser HL. Oculo-facio-cardio-dental (OFCD) syndrome. American Journal of Medical Genetics. 1996; 63(1):290-2. doi: 10.1002/(sici)1096-8628(19960503)63:1<290::aid-ajmg47>3.3.co;2-d
- Altug-Atac AT. Oculofaciocardiodental syndrome and orthodontics. American Journal of Orthodontics and Dentofacial Orthopedics. 2007; 131(1):83–8. doi: 10.1016/j.ajodo.2005.03.024
- Surapornsawasd T, Ogawa T, Tsuji M, Moriyama K. Erratum: Oculofaciocardiodental syndrome: Novel BCOR mutations and expression in dental cells. Journal of Human Genetics. 2015; 60(6):345. doi: 10.1038/jhg.2015.41
- Maden M, Savgat A, Görgül G. Radiculomegaly of permanent canines: Report of endodontic treatment in OFCD syndrome. International Endodontic Journal. 2010; 43(12):1152–61. doi: 10.1111/j.1365-2591.2010.01788.x
- Pace R, Giuliani V, Pagavino G. Endodontic management in oculo-facio-cardio-dental syndrome: A case report. Journal of Endodontics. 2011; 37(4):558-61. doi: 10.1016/j.joen.2010.12.015.
- Saberi EA, Ebrahimipour S. Evaluation of developmental dental anomalies in digital panoramic radiographs in Southeast Iranian Population. Journal of International Society of Preventive and Community Dentistry. 2016; 6(4):291-5. doi: 10.4103/2231 0762.186804.
- Ezoddini AF, Sheikhha MH, Ahmadi H. Prevalence of dental developmental anomalies: A radiographic study. Community Dental Health Journal. 2007; 24(3):140-4. PMID: 17958073.
- Larhant M, Sourice S, Grimaud F, Cordoba L, Leveau S, Huet P, et al. Giant canine with dentine anomalies in oculo-facio-cardio-dental syndrome. Journal of Cranio-Maxillofacial Surgery. 2014; 42(4):321–4. doi: 10.1016/j.jcms.2013.05.020
Type of Study: Original article |
Subject:
So on
Received: 2017/04/4 | Accepted: 2017/06/11 | Published: 2017/10/1
Received: 2017/04/4 | Accepted: 2017/06/11 | Published: 2017/10/1
References
1. Hayward JR. Cuspid gigantism. Oral Surgery, Oral Medicine, Oral Pathology. 1980; 49(6):500–1. doi: 10.1016/0030-4220(80)90070-5 [DOI:10.1016/0030-4220(80)90070-5]
2. Gorlin RJ, Marashi AH, Obwegeser HL. Oculo-facio-cardio-dental (OFCD) syndrome. American Journal of Medical Genetics. 1996; 63(1):290-2. doi: 10.1002/(sici)1096-8628(19960503)63:1<290::aid-ajmg47>3.3.co;2-d
https://doi.org/10.1002/(SICI)1096-8628(19960503)63:1<290::AID-AJMG47>3.3.CO;2-D [DOI:10.1002/(SICI)1096-8628(19960503)63:13.3.CO;2-D]
3. Altug-Atac AT. Oculofaciocardiodental syndrome and orthodontics. American Journal of Orthodontics and Dentofacial Orthopedics. 2007; 131(1):83–8. doi: 10.1016/j.ajodo.2005.03.024 [DOI:10.1016/j.ajodo.2005.03.024]
4. Surapornsawasd T, Ogawa T, Tsuji M, Moriyama K. Erratum: Oculofaciocardiodental syndrome: Novel BCOR mutations and expression in dental cells. Journal of Human Genetics. 2015; 60(6):345. doi: 10.1038/jhg.2015.41 [DOI:10.1038/jhg.2015.41]
5. Maden M, Savgat A, Görgül G. Radiculomegaly of permanent canines: Report of endodontic treatment in OFCD syndrome. International Endodontic Journal. 2010; 43(12):1152–61. doi: 10.1111/j.1365-2591.2010.01788.x [DOI:10.1111/j.1365-2591.2010.01788.x]
6. Pace R, Giuliani V, Pagavino G. Endodontic management in oculo-facio-cardio-dental syndrome: A case report. Journal of Endodontics. 2011; 37(4):558-61. doi: 10.1016/j.joen.2010.12.015. [DOI:10.1016/j.joen.2010.12.015]
7. Saberi EA, Ebrahimipour S. Evaluation of developmental dental anomalies in digital panoramic radiographs in Southeast Iranian Population. Journal of International Society of Preventive and Community Dentistry. 2016; 6(4):291-5. doi: 10.4103/2231 0762.186804.
8. Ezoddini AF, Sheikhha MH, Ahmadi H. Prevalence of dental developmental anomalies: A radiographic study. Community Dental Health Journal. 2007; 24(3):140-4. PMID: 17958073.
9. Larhant M, Sourice S, Grimaud F, Cordoba L, Leveau S, Huet P, et al. Giant canine with dentine anomalies in oculo-facio-cardio-dental syndrome. Journal of Cranio-Maxillofacial Surgery. 2014; 42(4):321–4. doi: 10.1016/j.jcms.2013.05.020 [DOI:10.1016/j.jcms.2013.05.020]
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
