
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://3dj.gums.ac.ir/article-1-252-en.html


Malignant Mucosal Melanoma of the Maxillary Sinus
Abstract
Malignant sinus mucosal melanoma is a rarely occurring melanoma in adults, with a poor prognosis. This study presents a rare case of a 33-year-old man suffering from headache and nasal obstruction for two weeks, and emphasizes the importance of immunohistochemical staining for diagnosis.
Key words: Melanoma, Paranasal Sinuses, Neoplasms
Case Report
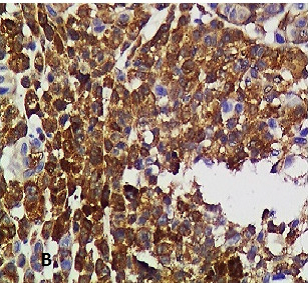
A 33-year-old man suffering from headache and nasal congestion for two weeks, consulted a private clinic, and complained of a 6-month constant swelling in the maxillary region after extraction of the right upper first molar tooth. The extra-oral examination revealed that the right orbit had displaced upward. The coronal CT scan showed a nearly 40 mm expansible mass lesion in the right maxillary sinus with an adjacent bony destruction especially in the inferio-lateral wall of the sinus. Moreover, observations revealed a bulge toward the right orbit, extension into the right nasal fossa, and opacification of the right anterior ethmoidal air cells. Mucosal thickening of both frontal sinuses and nasal septal deviation to the left was clear. An excisional biopsy was performed, wherein two irregular, firm, dark brown pieces of tissue measuring 6*4*1 mm in size were observed, with a solid and brown cut surface. After hematoxylin and eosin (H&E) staining, in a light microscopic view, sheets of round to oval cells with severe polymorphism, ill-defined cytoplasmic border, vesicular nuclei, atypical mitotic figures, and abundant apoptosis were seen; whereas, in some areas, spindleto-round view of neoplastic cells with eosinophilic cytoplasm was seen. Neoplastic tissue infiltration among bone trabeculae and muscles was apparent. Tissue necrosis with neoplastic cell aggregation was also evident around the artery walls; however, there was no evidence of tubular differentiation (Figure 1). The margin of neoplastic tissue was prominent. Respiratory epithelium with an infiltration of neoplastic cells was also observed occasionally. The clinical, radiographic, and microscopic differential diagnosis revealed sinonasal undifferentiated carcinoma and maxillary sinus carcinoma, with high grade malignant mesenchymal neoplasm suggestive of rhabdomyosarcoma and mucosal malignant melanoma. For a profound diagnosis, immunohistochemical staining was performed for HMB-45, vimentin, myogenin, and S100. Although the myogenin marker was negative, S100, HMB-45, and vimentin were positive (Figure 2). Due to specific immunostaining, final diagnosis revealed a malignant melanoma of maxillary sinus with diffuse infiltration of neoplasm into the soft tissue. The patient was subjected to radical surgical excision with lymph node dissection; however, after a 10-day-long follow up, he expired.
Discussion
Malignant sinus mucosal melanoma is a rare neoplasm occurring in the head and neck regions, with poor prognosis. According to previous studies, this neoplasm usually affects about 1 in 500,000 to 1 in 10,000,000 people.(1) This neoplasm has a multifactorial etiology, although a significant relationship was found between several carcinogens in the air, such as tobacco smoke, and increasing incidence of this type of neoplasm.(2,3) Some studies have stated minimal relation of alcohol and formaldehyde with this cancer. Axell et al., stated that there is a link between the chemical and physical stimuli and the mucosal pigmented lesions.(5) In the present study, there was no evidence of either opioids consumption/inhalation or other risk factors. Due to the specific area of the injury, invasiveness to the adjacent structures, and disability for early diagnosis, the 5-year survival rate of patients with this cancer is approximately between 5-30%.(3) Another reason for lack of early detection of lesion is symptom of injury that may be confused with some benign processes such as trauma, viral/
bacterial infection.(3) It is estimated that 60%–70% of cancers of the nasal cavity occur in the maxillary sinus, as seen in our case. Squamous cell carcinoma is the most commonly occurring neoplasm in the maxillary sinus, constituting about 70%–80% of cases, while malignant melanoma is responsible for about 0.4%–4% of malignancies in this region.(4) Mucosal melanoma of the head and neck regions is responsible for 0.72% of all melanomas; its mortality rate is higher than the cutaneous type melanoma.(2)
Age and gender do not affect the prognosis of the disease; this disease is more common in men than in women, with a ratio of 1.5: 1,(6,7) respectively, and it usually affects people aged above 45 years. Unlike the literatures, and as an interesting point of this report, in our case this disease occurred in a young man aged 33 years. In general, it is difficult to diagnose and treat neoplasms of the paranasal sinuses, due to the specific anatomical location of the melanoma,
which usually constitutes the paranasal sinuses and nasal cavity.(2) Therefore, no symptoms are generally seen in this disease until the tumor development disrupts the structure of the adjacent sinuses. Sinus tumors can invade the adjacent structures, as observed in our case, where the tumor invaded the orbit. Unfortunately, aggression and pressure on the eye and adjacent structures reoccur if effective intervention is delayed. Invasion of the orbit in advanced
stages could lead to loss of vision. Diagnostic assessment included clinical examination of the head and neck areas, such as face symmetry evaluation and vision strength test. Nasal cavity endoscopy can be useful for the diagnosis. Both CT and MRI imaging techniques can help with the diagnosis, but according to some sources, MRI imaging reveals the location of the tumor and its invasion into the surrounding tissues, more eminently.
Eventually, biopsy is the only effective way for diagnosis of this disease. After H&E staining, we performed three differential diagnoses comprising sinonasal undifferentiated carcinoma, high grade malignant mesenchymal neoplasm, and malignant melanoma. Although the presence of melanin pigmentation in maximum cases of malignant melanoma does not require immunohistochemical staining, in the present case there was no evidence of melanin pigmentation. Hence, we decided to perform an immunohistochemical staining for the definite diagnosis. Appropriate immunohistochemical markers for definite diagnosis of melanoma are HMB-45, Melan-A, S100, tyrosinase, and MITF. Melanoma strongly reacts with alpha subunit of S-100 protein, which is a calcium-binding protein found in neural tissue. The rate of reaction between the protein and melanoma is about 85%–100%. A more specific antigen of melanoma cells is HBM-45, which is a 100 kD glycoprotein, also known as premelanosome protein (Pmel). This antigen reacts with melanoma and junctional nevus cells.8 Staining appears to be more appropriate to lesions with pigment content compared to those with less pigmentation.(8)The sensitivity of HMB-45 has been proven to be 66%–97%, which decreased in metastatic lesions as compared to primary lesions.(8) Specificity of differentiating melanocytic tumors from nonmelanocytic tumors is 91%–100%. Sadly, HMB-45 has been shown to have decreased specificity for malignant melanoma in sentinel lymph nodes, in comparison with Melan-A;8 however, fortunately, HMB-45 represents poor sensitivity for diagnosing desmoplastic malignant melanoma.(8)
Melan-A, also known as MART-1, is another melanocyte differentiating antigen that is present in the cytoplasm of both melanocytes melanoma and retinal pigmented epithelium. According to some literatures, Melan-A is more sensitive than S100; however, this is still not proven. It is a less sensitive director for metastatic melanoma as compared to the primary one, but it is the most accurate marker for frozen section specimens.(8) For the case presented in this study, we chose melanoma markers (S100, HMB-45), mesenchymal neoplasms’ markers (vimentin, myogenin) to rule out the differential diagnosis. The case was positive for the first two markers and was negative for the latter. Finally, malignant mucosal melanoma was diagnosed by immunohistochemistry test.
Treatment for these lesions involves complete excision with adequate negative margins; nodal dissection should also be performed.(9)
Unfortunately, these tumors tend to spread radially to mucosal tissue and lymph nodes. Surgical neck dissection is indicated for lymph node metastasis in the neck region. The outcome of radiotherapy in the treatment of this lesion is not clear; however, some studies have shown a positive role of radiotherapy in the affected area.(10-13) Nevertheless, either radical surgical procedure or radiotherapy has been ineffective for increasing the survival rate of the patient.
Conclusion
Malignant melanoma of the paranasal sinuses is a rare and intricate disease, which presents with impaired vision, nasal obstruction, sinusitis, and epistaxis. Sadly, the prognosis remains poor and the diagnosis is still difficult. The critical point in dealing with such disease is early diagnosis in order to increase the survival rate of the patient.
References
1. Patel SG, Prasad ML, Escrig M, Singh B, Shaha AR, Kraus DH, et al. Primary mucosal malignant melanoma of the head and neck. Head Neck.2002;24(3):247-57.
2. Bhattacharya N. Survival and staging for non-squamous cell malignancies of the maxillary sinus. Arch of Otolarnygology Head Neck Surg.2003;129(3):34-7.
3. Gasparyan A, Amiri F, Safdieh J, Reid V, Cirincione E, Shah D. Malignant mucosal melanoma of the paranasal sinuses: Two case presentations. World J Clin Oncol.2011;2(10):344-7.
4. Berthelsen A, Andersen AP, Jensen TS, Hansen HS. Melanomas of the mucosa in the oral cavity and the upper respiratory passages. Cancer.1984;54(5):907-12.
5. Axell T, Hedin CA. Epidemiologic study of excessive oral melanin pigmentation with special reference to the influence of tobacco habits. Scand J Dent Res.1982;90(6):434-42.
6.Rapini RP, Golitz LE, Greer Jr RO, Krekorian EA, Poulson T. Primary malignant melanoma of the oral cavity. A review of 177 cases. Cancer.1985;55(7):1543-51.
7.Barker BF, Carpenter WM, Daniels TE, Kahn MA, Leider AS, Lozada-Nur F, et al. Oral mucosal melanomas: the WESTOP banff workshop proceedings. Western society of teachers of oral pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.1997;83(6):672-9.
8.Weinstein D, Leininger J, Hamby C, Safai B. Diagnostic and prognostic biomarkers in melanoma. J Clin Aesthet Dermatol. 2014;7(6):13-24.
9.Sun CZ, Chen YF, Jiang YE, Hu ZD, Yang AK, Song M. Treatment and prognosis of oral mucosal melanoma. Oral Oncol.2012;48(7):647-52.
10. Temam S, Mamelle G, Marandas P, Wibault P, Avril MF, Janot F, et al. Postoperative radiotherapy for primary mucosal melanoma of the head and neck. Cancer.2005;103:313-9.
11.Owens JM, Roberts DB, Myers JN. The role of postoperative adjuvant radiation therapy in the treatment of mucosal melanomas of the head and neck region. Arch Otolaryngol Head Neck Surg.2003;129:864-8.
12.Yanagi T, Mizoe JE, Hasegawa A, Takagi R, Bessho H, Onda T, et al. Mucosal malignant melanoma of the head and neck treated by carbon ion radiotherapy. Int J Radiat Oncol Biol Phys.2009;74:15-20.
13. Wu AJ, Gomez J, Zhung JE, Chan K, Gomez DR, Wolden SL, et al. Radiotherapy after surgical resection for head and
neck mucosal melanoma. Am J Clin Oncol.2010;33:281-5.
Figure 1. H&E staining reveals round to oval malignant neoplastic cells, ×40
{kind=link}
Figure 2. A. Positive HMB45 immunohistochemical staining. B. Positive vimentin Immunohistochemical staining, ×40
{kind=link}
{kind=link}
Received: 2017/02/21 | Accepted: 2017/02/21 | Published: 2017/02/21
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
