
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://3dj.gums.ac.ir/article-1-236-en.html

 , Nazanin Bashardoost2 , Narges Kakaei * 3, Alireza Ansari4 , Zahra Poorhabibi5 , Reza Modanloo Jouibary6
, Nazanin Bashardoost2 , Narges Kakaei * 3, Alireza Ansari4 , Zahra Poorhabibi5 , Reza Modanloo Jouibary6
2- Department of Oral and Maxillofacial Pathology, Guilan University of Medical Sciences, Rasht, Iran
3- Guilan University of Medical Sciences-International Branch, Research Committee Member
4- Guilan University of Medical Sciences-International Branch
5- Guilan University of Medical Sciences, Rasht, Iran
6- Guilan University of Medical Sciences
Histopathological Study of the Effect of Smoking on Free Gingiva in Patients with Moderate to Severe Chronic Periodontitis
Abstract
Introduction:
Cigarette smoking is a risk factor for progression of periodontitis, which effects on the incidence, extent and severity of the periodontal disease and no other known factors can be harmful as much as smoking to the periodontal tissues. The purpose of this study was to determine clinical and histopathological effects of smoking on free gingiva in smokers and non-smokers with chronic periodontitis.
Materials and Methods:
Biopsies were obtained from palatal gingiva of first and second molar of 72 patients with chronic periodontitis (36 smokers and 36 non-smokers). These samples were sent to the pathologic laboratory for microscopic examinations, and then the data were analyzed by SPSS version 21.
Results:
Histopathological examination showed that smoking increase the thickness of the outer and inner epithelium of free gingiva, Collagenized connective tissue, and CAL; and decrease the vascular density.
Conclusion:
It seems that the reduction of the clinical signs of inflammation in the gingival tissue of smokers are because of changes in gingival epithelium and connective tissue due to smoking.
Key words:
•Gingiva •Periodontitis •Smoking.
Introduction
Today, cigarette smoking and tobacco use are considered as one of the greatest threats to human health in the world.(1) According to the World Health Organization (WHO), annual tobacco consumption results in an average of 4.5 million deaths in the world.(1) Tobacco use is the most important factor for deaths in more than two-thirds of people in developing countries, resulting in more premature deaths due to tobacco use than those due to HIV, tuberculosis, and birth complications.(2) Dependence on tobacco products such as cigarettes is chronic and dangerous.(1) Cigarette smoke contains more than 3800 chemicals, including carbon monoxide, hydrogen cyanide, and oxidizing radicals (1-3), and 60 of these chemicals are known as carcinogens or suspected carcinogens.(1-3) Tobacco smoke contains carbon monoxide, thiophosphate, hydrogen cyanide, and nicotine and its metabolites.(1-3)
Nicotine is a substance that causes people to become addict to smoking.(1-3)
Smoking harms nearly every organ of the body, causing several diseases and reducing the general health; hence the immediate withdrawal of smoking has long-term benefits and in general improves the body health.(3) Some of the diseases caused due to smoking are abdominal aortic aneurysm, acute myeloid leukemia, cataract, cervical cancer, kidney cancer, pancreatic cancer, pneumonia, periodontitis, and stomach cancer, in addition to previously known diseases such as cancers of the bladder, esophagus, larynx, lung, mouth, and throat, and chronic lung disease, coronary heart disease, cardiovascular disease, and sudden infant death syndrome.(3)
A strong association between smoking and periodontal diseases, alveolar bone loss, tooth mobility, increase in probing depth, and tooth loss has been reported more significantly in smokers than in non-smokers.(1) The effect of smoking on the periodontal tissue is dependent on the dose and duration of use.(1) Studies show that 40% of chronic periodontitis may be attributed to smoking.(1) Periodontitis is an inflammatory disease of the teeth-supporting tissues and is considered as an opportunistic infection caused by a microorganism or a group of specific microorganisms and causes progressive destruction of the periodontal ligament and alveolar bone, which is associated with pocket formation or gingival recession or both.(2,3) According to the WHO
reports, periodontitis is the most commonly known disease in humans in most parts of the world, with a high prevalence, so that almost half of the children and almost all adults are also affected.(4) The early stage of the disease is gingivitis, in which the junctional epithelium remains on its initial position on the teeth.(5) If the inflammatory process involves gums and the periodontium and periodontal attachment loss has occurred, this condition should then be defined as the so-called periodontitis.(6) The most common form of periodontitis is chronic periodontitis, which is associated with plaque formation and progresses at a slow to moderate rate, but severe destructive courses may also be encompassed.(2,3)
Disease progression rate can be influenced by
local, systemic, or environmental factors that are affected by the host–bacterial natural reaction.(2,3)
Clinical attachment loss (CAL) is the clinical appearance detected in periodontitis and not in gingivitis.(7) It usually connected with pocket formation, density changes, and changes in the adjacent alveolar bone height.(7)
Periodontitis can be divided into three forms of chronic periodontitis, aggressive periodontitis, and periodontitis as a manifestation of systemic disease.(7) Periodontitis is not an age-related disease, but an age-associated disease.(7) The severity of the disease can be mild, moderate, and severe; CAL of 1-2 mm indicates mild damage, CAL of 3-4 mm suggests moderate damage, and CAL of 5 mm indicates severe damage.(6)
Smoking is common in low-income adults, more than that in middle- or high-income adults, whereas it is less in people with higher levels of education.(6) Evidence shows that regardless of age, sex, and plaque index, smokers and ex-smokers are 7.2 and 3.2 times more likely to develop periodontal disease than non-smokers, respectively, and that smoking can affect the periodontal tissue more in men than in women.(8)
Several studies have been done on smokers and found that there is no difference in plaque formation compared with non-smokers, which indicates that if changes such as loss of alveolar bone of compromised periodontal condition and increased number of missing teeth have
occurred, it contributes to qualitative changes in the plaque, not to qualitative changes.(5) On the other hand, a smoker’s microvascular system in comparison with non-smokers exhibits significant changes in blood flow that lead to reduction of the clinical signs of inflammation.(5) As a result, smokers have less bleeding during probing than non-smokers.(5) Attachment loss and alveolar bone loss are more common in smokers.(5) Although the exact mechanism is not known, the effects of smoking on periodontal status, the host response to bacterial plaque, and the wound healing response in the host can have significant effects.(6) Most of these disorders affect blood vessels and their function, namely their ability to deliver oxygen, nutrients, and growth stimulants of tissues.(6) Even a slight change in the arteries can have significant effects on tissues and reduce the treatment response in smokers.(6)Smokers do not respond to mechanical treatment compared to non-smokers, due to the high levels of microorganisms such as Aggregatibacter actinomycetem comitans, Tannerella forsythia, and Porphyromonas gingivalis in post-treatment, and the bacterial level is higher in smokers.(9) There are several components in tobacco smoke that may be associated with immunosuppression.(3)Smoking primarily causes a change in the host response to the pathogens in the periodontal
tissue so that the impact on mechanisms leads to destruction of the surrounding healthy gum tissue.(3)
In smokers, the number of neutrophils in the systemic circulation is increased, while these cell numbers are reduced in the gingival sulcus.(3) Smoking also affects their performance so that it impairs neutrophil chemotaxis and phagocytosis.(3) Probably there are some carcinogenic substances in cigarette smoke that are involved in the etiology of mouth neoplasia.(10) Because of the lack of clear findings regarding the process of tissue changes in chronic periodontitis in smokers, and given the large number of smokers in the country, and also as regards that the oral cavity is the first part of the body exposed to cigarette smoke, we investigated the histopathological effect of smoking on free gingiva in smoker patients with moderate to severe chronic periodontitis in comparison with non-smokers.
Materials and Methods
This was a case-control study in which the effect of smoking on palatal gingiva of teeth 6 and 7 in 72 patients with moderate to advanced chronic periodontitis (attachment loss >3 mm) referred to Guilan Dental School was analyzed. Half of them were (n = 36) smokers and the other half (n = 36) were non-smokers. In this study, the sampling method was simple sampling. Heavy smokers were analyzed according to the Centers for Disease Control and Prevention (CDC) criteria.
Pregnant women, people who had used substances other than cigarettes and other drugs, and all people with a systemic disease were excluded from our study. Data were collected before the start of surgical periodontal treatment and included demographic data, patient’s smoking or non-smoking status, smoking and its duration (according to the patient’s statements), surgical area probing depth, surgical area’s CAL, the average thickness of stratum corneum, the average thickness of the inner and outer epithelium in the maximum and minimum thickness, connective tissue collagenization, and blood vessels in each area. Probing depth of the area where the gum tissue was removed during surgery was measured. All patients underwent undisplaced flap surgery, and part of the palatal gingival collar 6 and 7 maxillary teeth were removed and collected as a sample.
Samples collected from the patients were placed in 10% formalin for fixation for at least 24 h and were then sent to the pathology laboratory in the private sector. After the usual procedure, paraffin blocks of specimens were prepared. Then, 5-μm-thickness paraffin blocks were cut and stained in the usual manner with hematoxylin eosin (H&E). After mounting the specimens on a glass slide and drying, the specimens were ready for light microscopy examination. First, three to six microscopic images were taken with a magnification of 10× from each slide, which included the maximum thickness of the internal and external epithelium areas and the minimum area and the stratum corneum. Measurement was performed at three points in any point, and the average size for areas with a maximum and a minimum thickness of the epithelium and stratum corneum was expressed. Collagenization of the connective tissue was also observed and recorded. In addition, the number of blood vessels was observed with 40× magnification in three areas. After microscopic examination, the results were recorded on the questionnaire for each patient, and the data were analyzed by one-sample, Smirnov test, Pearson correlation, and linear regression, with significance set at P < 0.05.
Results
This study was performed on 72 tissue samples obtained from72 patients, including 44 men (61.1%) with an average age of 47.5±5.12 years and 28 women (38.9%) with an average age of 44.84±5.12 years. The overall average age of both groups was 46.31±5.22, with a range of 59–36 years. There was no statistically significant difference between the two groups according to age. The smoker group included 26 men and 10 women, and the non-smoker group included 18 men and 18 women. (Table 1) Based on the research findings, in both smokers and non-smokers, there was no statistically significant difference in terms of age, pocket depth, and minimum thickness of the outer epithelium. However, regarding CAL, the maximum thickness of the inner and outer epithelium, minimum thickness of the inner epithelium, stratum corneum thickness, and capillary density showed a statistically significant difference between the two groups. (Figure 1 and 2)
Because of the qualitatively of collagenization variable, we analyzed it separately, so that collagenized connective tissue was observed in 21 men (80.7% of smoker men) and 7 women (70% of smoker women), and also in 4 men (22.2% of non-smoker men) and 4 women (22.2% of non-smoker women). Collagenized connective tissue was not observed in 5 men (19.3% of
smoker men) and 3 women (30% of smoker women), and in 14 men (77.8% of non-smoker men) and 14 women (77.8% of non-smoker women). Collagenization of the connective tissue was more significant in smokers than in non-smokers (P < 0.001) (Figure 3). In the both non-smoking group collagenization of connective tissue of 8 cases (22.2%) was observed, while in the both smoker group at 8 cases (22.2%) was not
observed. (Table 2)
According to Table 1, regarding the correlation between age and gender and smoking, a statistically significant difference was observed among the variables capillary density, CAL, stratum corneum thickness, maximum and minimum thickness of the inner epithelium, and maximum thickness of the outer epithelium in relation to cigarette smoking. In addition, a statistically significant difference was observed among the variables pocket depth, stratum corneum thickness, maximum and minimum thickness of the outer epithelium in relation to gender. Finally, the linear model test stepwise method showed that the maximum and minimum thickness of the inner epithelium and CAL, with odds of 0.061, 0.129, 0.139, and 0.137, were the only effective variables, but they did not have any predictive power, because the significance level was more than 0.05.
Discussion
Smoking is one of human’s health risks with a widespread prevalence, which causes serious risks.(4) Some of the harmful effects of tobacco include reduced blood flow, tissue hypoxia, collagen deposition, prostacyclin formation,
impaired polymorphonuclear neutrophil function, increased fibrinogen, increased blood
viscosity, and increased systemic epinephrine and norepinephrine levels. In fact, the stomatogastric system generally suffers from the effects of tobacco byproducts.(11)
This study investigated the histopathological and clinical effects of smoking on free gingiva using a sample size of 72 patients with moderate to advanced chronic periodontitis.
The results of this study showed that CAL was significantly higher in smokers than in nonsmokers, while the probing depth between the two groups showed no significant difference (probing depth was slightly higher in non-smokers than in smokers, but the difference was not
significant). The results of studies done by Gunsolley et al. (12), Thomson et al. (13), Souza et al. (14), Sreedevi et al. (10), and Anand et al. (15) were similar to our results, and also regarding the pocket depth, the results of our study were similar to those reported by Bouclin et al.(16)
In this study, the maximum thickness of the inner and outer epithelium and the minimum thickness of the inner epithelium were significantly higher in smokers than in non-smokers. Although the minimum thickness in the areas of the outer epithelium was greater in smokers, the difference was not significant. In general, the thickness of the inner and outer epithelium of smokers was significantly higher, which was similar to the result reported by Titta et al. (17) and Bajagic et al. (18), while Villar et al. (19) and Gultekin et al. (4) did not find significant differences in the epithelium thickness between smokers and non-smokers. This difference could be due to the more number of cases in the present study and the samples being obtained from the palate, solely, which is mostly affected by cigarette smoke, whereas in the other studies, the samples were obtained from different parts of the mouth.
The vessel density in non-smokers was significantly higher than that of smokers in this study, whereas Lindeboom et al. (20) reported no significant difference between the two groups, and Rahman et al. (21) reported increased density of blood vessels in smokers. This difference could again be due to the more number of cases in this study than the study by Rahman et al.(21)
In this study, the amount of connective tissue collagenization was significantly higher in
smokers than in non-smokers, which is in accordance with the results of Bouclin et al. study (16), whereas Titta et al. (17) reported less connective tissue collagenization in smokers due to the consumption of fumigant tobacco. Smokers’ stratum corneum thickness was significantly higher than that in non-smokers in this study, which is similar to the result of studies by Titta et al.(17), Saebi et al.(22), Villar et al.(19), Bajagic et al (18), and Gultekin et al.(4) In this study, in general, the thickness of the inner and outer epithelium, stratum corneum thickness, the amount of connective tissue collagenization, and CAL were higher in smokers than in non-smokers; however, vessel density was higher in non-smokers than in smokers. The results of this study and other similar studies demonstrate that cigarette smoking has harmful effects on the periodontium and oral mucosa. Regarding the high prevalence of oral cancer in smokers, it is suggested that dentists must remind the patients about the oral problems caused by smoking and encourage them to abandon the habit of smoking.
Acknowledgments
This article was written based on the thesis work of Reza Modanloo Jouibary done in the Guilan University of Medical Sciences. We thank Guilan University of Medical Sciences for their technical support.
References
1. Zee K. Smoking and periodontal disease. Aust Dent J.2009; 54(1): 44–50.
2. Carranza F, Newman M, Takei H, Klokkevold P. Carranza’s Clinical Periodontology.10th Ed. St Louis: Saunders; 2006.p. 46-67,100-9,251-9.
3. Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999; 4(1):1-6.
4. Gültekin SE, Sengüven B, Karaduman B. The effect of smoking on epithelial proliferation in healthy and periodontally diseased marginal gingival epithelium. J Periodontol. 2008; 79(8):1444-1450.
5. Highfield J. Diagnosis and classification of periodontal disease. Aust Dent J. 2009; 54(1): 11–26.
6. Ana Pejčić, Radmila Obradović, Ljiljana Kesić, Draginja Kojović Smoking and Periodontal Disease a Review. Facta universitaitis. 2007; 14(2): 53-59.
7. Jonson GK, Hill M. Cigarette smoking and the periodontal patient. J Periodontol. 2004;75(2):196-209.
8. Rosa GM, Lucas GQ, Lucas ON.Cigarette smoking and alveolar bone in young adults: a study using digitized radiographs, J Periodontol. 2008;79(2):232-44. doi: 10.1902/jop.2008.060522.
9. Malhotra R, Kapoor A, Grover V, Kaushal S. Nicotine and periodontal tissues. J Indian Soc Periodontol. 2010; 14(1): 72–9.
10. Maddipati S, Alampalli R, Chini D. Periodontal Status in Smokers and Nonsmokers: A Clinical,Microbiological, and Histopathological Study. International Journal of Dentistry.2011; 21(10):1-10.
11. Misch CE, Resnik RR. Medical Evaluation of the Dental Implant. contemporary implant dentistry. 2008:476-477.
12. Gunsolley JC , Quinn SM , Tew J , Gooss CM ,Brooks CN , Schenkein HA . The effect of smoking on individuals with minimal periodontal destruction. J Periodontol 1998;69(2):165-70
13. Thomson WM, Poulton R, Broadbent JM, Moffitt TE, Caspi A, Beck JD. Cannabis Smoking and Periodontal Disease Among Young Adults. JAMA. 2008; 299(5): 525–531.
14. Burgan SZ. Smoking behavior and views of Jordanian dentists: A pilot survey.Oral SurgOral Med Oral Pathol Oral Radiol Endod 2003; 95(2 ): 163-8
15. Anand PS, Kamath KP , Bansal A , Dwivedi S , Anil S . Comparison of periodontal destruction patterns among patients with and without the habit of smokeless tobacco use--a retrospective study. J Periodontal Res 2013;48(5):623-3.
16. Bouclin R, Landry RG, Noreau G. The effect of smoking on periodontal structure review. J Canadian Dent Assoc. 1997; 63(5): 356-63.
17. Luomanen M, Tiitta O, Heikinheimo K, Heinaro I , Happonen R. Effect of snuff on cytokeratin expression in oral vestibular sulcus epithelium. J Oral Pathol Med 1997; 26(3): 110–6.
18. Bajagic V, Pejcic A, Zivkovic V, Petrovic A. Histochemical study of gingival epithelium in smokers and non- smokers. Acta Facultatis Medicae Naissensis. 2006; 23(3):151-4.
19. Villar CC, de Lima AF. Smoking influences on the thickness of marginal gingival epithelium. Pesqui Odontol Bras. 2003;17(1):41-5.
20. Lindeboom JA, Mathura KR, Harkisoen S, vanden Akker HP. Effect of smoking on the gingival capillary density: assessment of gingival capillary density with orthogonal polarization spectral imaging. J Clin Periodontol. 2005; 32(12): 1208–12.
21. Rahman BU, Rahman MM, Arsalan A. The effect of cigarette smoking on human gingival tissues. J Pak Med Assoc. 1994; 44(9):210-2.
22. Saebi KH, Eslami B, Fathieh A, Poorsepanj G. The effect of smoking on sulcular epithelial keratosis. Beheshti Univ Dent J. 2003;21(1):22-30.
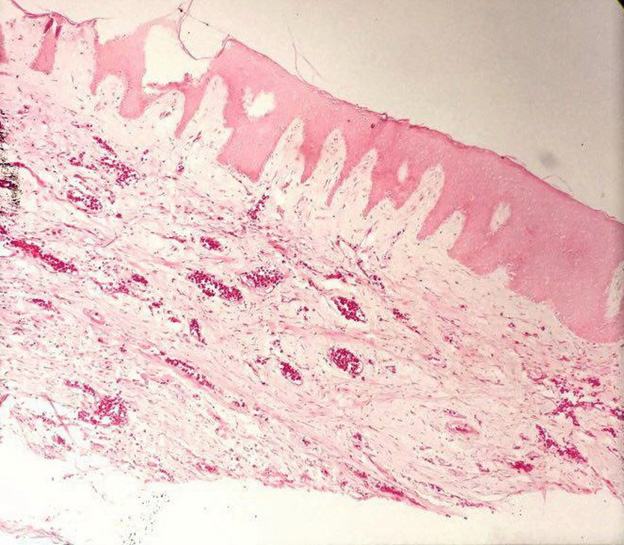
Figure 1. H&E staining shows higher vessel density in non-smokers x10
./files/site1/files/1%282%29.png
{kind=link}
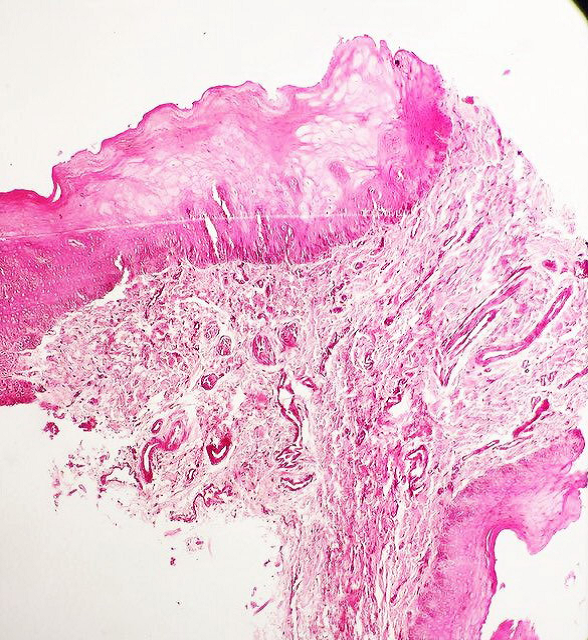
Figure 2. H&E staining shows higher connective tissue collagenization smokers x10
./files/site1/files/2%282%29.png
{kind=link}
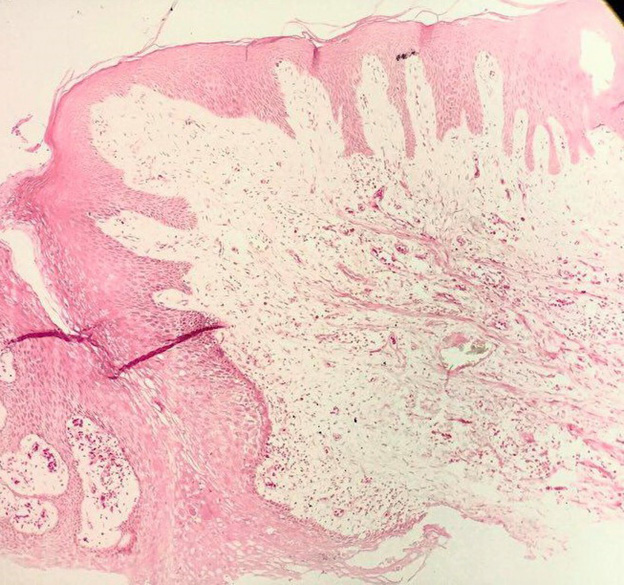
Figure 3. H&E staining shows higher thickness of epithelium in smokers x10
./files/site1/files/3%281%29.png
{kind=link}
Table 1. Pearson correlation or quantitative variables
|
Variables |
Capillary |
Pocket |
CAL |
Stratum |
Maximum |
Maximum |
Minimum |
Minimum |
CT |
|
|
Age |
PC |
-0.23 |
0.06 |
0.19 |
0.03 |
0.15 |
0.11 |
0.15 |
0.02 |
-0.21 |
|
P-value |
0.08 |
0.59 |
0.11 |
0.77 |
0.20 |
0.36 |
0.22 |
0.89 |
0.08 |
|
|
Gender |
PC |
0.16 |
0.23* |
-0.14 |
-0.32** |
-0.15 |
-0.28* |
-0.21 |
0.35* |
0.17 |
|
P-value |
0.23 |
0.048 |
0.23 |
0.007 |
0.19 |
0.002 |
0.07 |
0.003 |
0.15 |
|
|
Smoker |
PC |
0.62 |
0.22 |
0.44 |
0.72** |
0.56 |
0.61** |
0.62* |
0.17 |
0.56** |
|
P-value |
0.001 |
0.06 |
0.001 |
0.001 |
0.001 |
0.001 |
0.001 |
0.15 |
0.001 |
**This relationship in a pair of ranges, P < 0.01, is significant.
*The relationship in a pair of ranges, P < 0.05, is significant.
Table 2. The Effect of demographic variables on the dependent variables
|
Variables |
Beta |
t |
P-valuet |
|
Age |
0.339 |
- |
0.005 |
|
Gender |
0.082 |
- |
0.487 |
|
Stratum corneum thickness |
0.712 |
-8.566 |
0.001 |
|
Maximum thickness of inner epithelium |
0.545 |
-5.202-5.202001 |
0.001 |
|
Maximum thickness of outer epithelium |
0.585 |
-5.956 |
0.001 |
|
Minimum thickness of inner epithelium |
0.606 |
-6.151 |
0.001 |
|
Minimum thickness of outer epithelium |
0.112 |
-0.951 |
0.345 |
|
CT collagen ization |
0.610 |
5.594 |
0.001 |
|
Capillary density |
0.528 |
5.064 |
0.001 |
|
Pocket depth |
0.205 |
1.712 |
0.092 |
|
CAL |
0.414 |
-3.666 |
0.001 |
Received: 2016/12/6 | Accepted: 2016/12/6 | Published: 2016/12/6
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
The end of professor Samii Blv, Guilan University of Medical Sciences Complex, Dental School, Rasht, Iran.
Journal Tel : +9813 33486428
Publisher Tel : +9821 86037228 , 86036497
Email: den3djournal@gums.ac.ir
